Case Introduction
Thank you so much for having me. I want to introduce you to our case.
- Patrick: 7 y.o. male in 2nd grade that has difficulties with reading, completing homework, and the following instruction during school occupations. He does not finish copying things from the board and tends to have difficulty with writing, coloring, and ball sports. He uses his finger to read, loses his place, and often complains he can’t find things in his books. He is slow with dressing routines, buttons and fasteners are a “nightmare”, and cleaning his room is tough.
- He lives with his mother and father and two siblings. He is a shy child who loves dinosaurs, football, and Avengers. He says he wants to be a firefighter when he grows up, like his father.
- Patrick was a normal delivery without complications. Mom reports he was a fussy baby with colic. She also indicates that he was slow with some developmental motor milestones, particularly balance-related and object manipulation. She said he has always had difficulty following directions and struggles with ADLs. She calls him “clumsy”.
- Patrick also has a history of ear infections and adenoid removal. He is on his second round of ear tubes.
Today, I am doing a case study format. I want to give you a conceptual way to think about how to intervene with a child who has visual challenges that are affecting school performance, ADL performance, or play performance. Patrick is a seven-year-old male in second grade. He has difficulties with reading, completing his homework, and following instructions during his school occupation. He does not finish copying things from the board and tends to have difficulty with writing, coloring, and ball sports. He uses his finger to read, loses his place, and often complains that he cannot find things in his book. He is slow with dressing routines, and buttons and fasteners are a nightmare. He also has a tough time cleaning his room. He lives with his mother, father, and two siblings. He is a shy child who loves dinosaurs, football, and Avengers and says he wants to be a firefighter when he grows up just like his dad. Patrick was a normal delivery without complications, but mom reports he was a fussy baby with colic. She also indicates that he was slow with some developmental milestones related to motor, particularly balance-related ones, and object manipulation. She said that he has always had difficulty following directions and struggles with his ADLs. She calls him clumsy. Patrick has a history of ear infections and adenoid removal, and he is on the second round of ear tubes. This scenario might sound familiar to many of you. This is typical of a lot of the kids that I see. These are "clumsy kids" who have some difficulty in school, and it can often be misconstrued as behavioral. And, if you know Patrick, he is a really sweet kid and he is not behavioral at all.
Vision
- The total process responsible for reception and cognition of visual stimuli
- Reception=sensory functions
- Extract, organize info from environment
- AKA: oculomotor skills, visual motor skills
- Reception=sensory functions
- Cognition=specific mental functions
- Interpretation of what is seen
- AKA: visual perceptual skills, visual cognitive skills
I want to start out with defining vision. It is the total process of receiving information and then processing it cognitively. It a very complicated process. How we receive information is related to sensory functions. We have to extract information from the environment. For example, in order for you to take a picture, you have to move your phone camera to the right spot. With a selfie, you might realize that you are cutting off people's heads. You have to angle it the right way to get everyone in the picture. That is an example of reception. You have to make sure that you can actually receive that information. We also refer to this as oculomotor skills or visual-motor skills. This is especially true with vision. Cognition, on the other hand, is the mental functions involved with vision. This is interpreting what is seen and that becomes much more subjective. We could call these visual perceptual skills or visual cognitive skills. Back to our picture metaphor, we look at the picture on our phone in order to process it. These are two different things, but they are very much dependent on each other. Part of the challenge I think in our profession when trying to assess someone is that they use a lot of things synonymously.
Functions
- 5 functions of the mature visual system:
- Respond and adjust to retinal stimuli
- Anatomic, physiologic
- Move both head and eyes to collect raw data (reading, copying, taking tests)*
- Oculomotor, vestibulo-ocular control
- Effectively interpret visual information
- Visual perceptual skills
- Respond to visual cues through efficient limb movements
- Visual-motor integration
- THEN…Integrate the above functions in occupations
- Respond and adjust to retinal stimuli
When we think about visual function, this is talking about visual acuity, visual fields, contrast sensitivity, etc. These are the basic functions of vision. However, you can also talk about "functional vision." Functional vision is how we use it. This focuses on ocular motor skills and how we use the two eyes together. Not only do we have to move each eye, but we also need to be able to move them together. On top of that, we have to be able to accommodate or adjust the eyes for near and far stimuli. Accommodation is sort of separate from traditional oculomotor skills because accommodation requires the integration of your lens and your ciliary muscle. Thus, when I am talking about oculomotor skills, I am not talking about accommodation. For me, the only way to really make a change in accommodation is vision therapy. When I have kids that have accommodation issues, I send them straight to vision therapy because the ciliary muscle is smooth muscle, and it is much more challenging to affect change in that. The oculomotor skills that I am talking about are things like convergence, divergence, saccades, tracking, and smooth pursuits.
What are the five functions of a mature visual system? It starts with basic anatomy and physiology. Then, we have to have oculomotor and vestibulo-ocular control. Can I move both my head and my eyes to collect that data? Sometimes the eyes move with the head, and sometimes the eyes move by themselves and do more subtle movements. Some of our kids might struggle with that operation and need to use their whole body to move with their eyes because they have difficulty with that dissociation. Next, we need to effectively interpret visual information. This is where we start to move into the cognitive piece or visual perceptual skills. We then respond to visual cues by moving our limbs for visual-motor integration. Finally, all of this is integrated into occupations. There is a hierarchy of development. Visual-motor integration is extremely complex and a lot of times our kids are missing some of these lower-level functions.
Visual Development
Here is a great link on visual development to review on your own. It is a really cool video.
Skeffington's Model
I also want to introduce to you Skeffington's model shown in Figure 1.
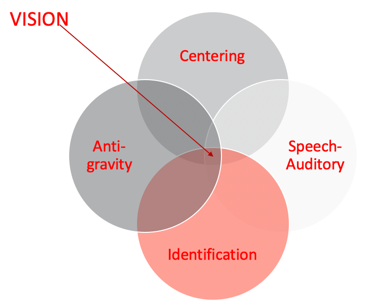
Figure 1. Skeffington's model.
I do not know how many of you are familiar with Skeffington's Model. When I started working at the university, I did program development over at the middle school. My background is in brain injury. Now I work with kids who have similar issues with visual abilities and function as well as some struggles with attention in school. I have always worked with optometrists and have had an interest in vision. Optometrists introduced me to Skeffington's model, and it helped me to understand why some of the things that I had been taught and was using with my clients was not working.
- Antigravity system (vestibular system)
- Internal balance
- Centering
- Attention and orientation
- Directing body, head, eyes toward an area in space
- Identification
- Gathering meaning from areas of selected attention in external space
- Relationships between details (discrimination and differentiation)
- Speech-auditory
- Analysis and communication of what is seen
Among these four circles, not one is more important than the other. They all need to be balanced. First is the antigravity system or the vestibular system. You cannot think about vision without thinking about the vestibular system. We need an internal balance for postural control. And, postural control is really essential to attending to our environment. There is also a huge relationship between the vestibular system and eye movements. The vestibular ocular reflex helps the body moves to right itself.
Centering is the idea of using attention and orientation to direct your body, head, and eyes towards something in space so you can receive information. Do I have the control to orient to something, attend to it, and dissociate as I need? There has to be underlying proprioceptive function, as well as strength, to be able to do something. The strength either needs to be internal or via external supports.
Identification was one of the pieces I was missing when I was doing a lot of the visual work in the past. Identification is gathering meaning from whatever you are attending to in space and starting to appreciate the relationships between the details. This becomes really important when processing information. These visual perceptual skills help to discriminate and differentiate between things. We are not just talking about being able to label something but label it in a way where you can tell the differences and the little nuances between things that lead to higher-level thinking and awareness.
The speech and auditory area is the ability to analyze and communicate what I am seeing. This is more of a cognitive language piece. This requires the parietal lobe functioning to bring in spatial relation or position in space. I really cannot do that functionally if I do not know that I have two sides of my body or that the right and left sides can do two different things at the same time or together. Can I cross the midline? These things inform my position in space and spatial relations. If I do not understand right versus left on myself or with a person sitting across from me who is giving me directions, I have a problem. I cannot really discriminate and differentiate how to get there from my own perspective, much less yours. This starts to make sense why this is extremely important for visual processing.
Skeffington's model tells us that we see with our whole body.
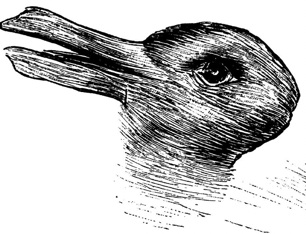
Figure 2. Optical illusion.
Figure 2 is an example of an optical illusion. Some of you might see one animal, while some of you might see another. I will give you a second to see if you can figure it out. Some of you might see both rather quickly, while others only see the one animal. some of you might struggle to see both the rabbit and the duck. Identification informs our visual perceptual skills to be somewhat subjective.
Second Grade Occupations
Our friend Patrick is in second grade. What is expected of a second-grader? Figure 3 is an overview.
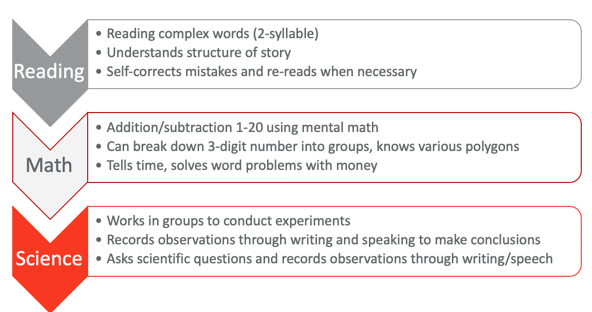
Figure 3. Overview of 2nd-grade occupations.
These are the universal standards for second grade. They should be able to read complex words which means two-syllable words, understand the structure of a story, self-correct mistakes, and reread when necessary. Those are pretty high-level reading skills. In math, they should be able to add and subtract one through 20 using mental math. I know some adults that struggle with that. They can break down three-digit numbers into groups into ones, tens, or hundreds. They also know various polygons, which would then indicate that they have some awareness of visual discrimination and form constancy starting to develop. They can tell time with an analog clock. You can put an asterisk next to that just from societal changes with technology. They still should be able to in theory to read a clock. They should be able to solve word problems with money, start to manipulate money and coins with some basic adding, and things like that. From a science perspective, they should be able to work in groups to conduct simple experiments. They should also be able to record their observations through writing and speaking to make conclusions about what they have observed. They should also be able to ask scientific questions and record observations throughout the process, not just at the end. What is kind of interesting here about the science piece is that this is universal. This scientific inquiry could be used for other topics as well.
Visual Development
From a visual development standpoint, I cannot emphasize enough how important this hierarchy is in Figure 4.
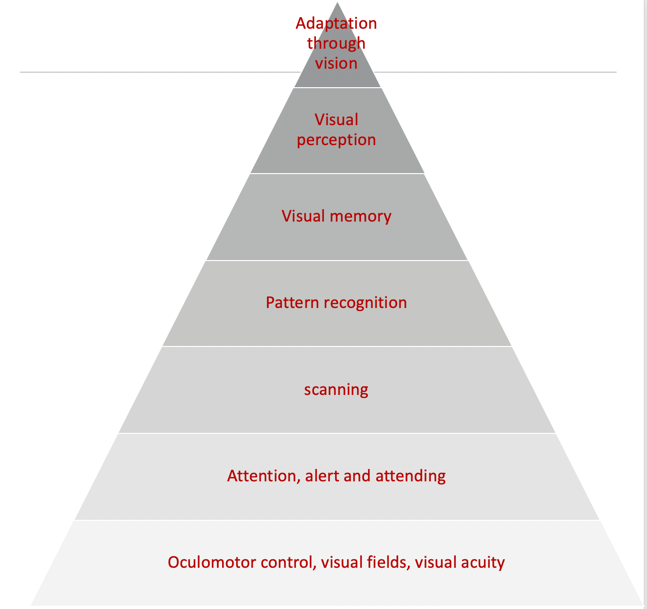
Figure 4. Visual hierarchy.
I am going to go through it rather quickly, but I want to point out the base of it all is oculomotor control. Once the oculomotor control is there, then there is visual attention as well as vigilance or a persistence toward it. If I am really looking at something to figure it out, I have to have some persistence. Once I can attend to something, the next levels are scanning and pattern recognition. Visual memory starts to kick in once patterns are recognized. With visual memories, this becomes functional visual perception. These are perceptual skills like visual closure, discrimination, spatial relations, position in space, figure-ground, and topographical orientation. These are all higher-level visual perceptual skills that we all test all the time. Once you get through all these levels, the final area is adaptation through vision.
I always use this analogy because in Florida we have hurricanes. One of the big things down here is to get hurricane windows. Hurricane windows are great because they can withstand the impact of debris flying around during a hurricane. So, if you have a strong foundation and hurricane windows, you are kind of safe from the storm or even a tornado. However, if you have a mobile home or a tiny house, even if you add hurricane windows, the whole house will blow away during the storm without a proper foundation. I think about this with our kids as well. Many of our tools are related to visual perception. Back in the day, I would start treatment with something like mazes for visual perception or handwriting for visual-motor integration without going back and appreciating that the child was missing a foundational element. We want to make sure that they have those foundational pieces.
Case Assessment Results
- Assessments: M-FUN, DTVP-3, Beery VMI, oculomotor screening,
- School reports: Below age range in reading, above age range in math, handwriting difficulties, sits in front due to difficulty following directions, no significant behavior concerns but slow with work and often doesn’t complete assignments
- Dislikes PE, but enjoys music, art, and science
For Patrick, I used the M-FUN (Miller Function and Participation Scales), the DTVP-3 (Developmental Test of Visual Perception), the Beery VMI (Beery-Buktenica Developmental Test of Visual-Motor Integration), and oculomotor screening. I also completed the SFA, which is the School Function Assessment. I used these because I wanted to get some information about vestibular functioning. I also wanted to a sensory profile and take a look at his motor and visual skills as well as non-motor and visual skills (DTVP-3). Oculomotor testing is also important. I often just do tracking kinds of things. I love the King-Devick Test for saccades. There is also the Developmental Eye Movement Test, the DEM, which is also very helpful. I do not know what you have access to, but you can do oculomotor testing just through the basic screenings that you do.
From his school reports, I saw that he was below the age range in reading, which we kind of suspected anyway, but he was above age range in math. He had some handwriting difficulties according to the teacher. She felt that he was slow, and it took him a long time and a lot of effort. She had him sitting in the front because he had such a hard time following directions. He was always kind of behind. His teacher did not feel that he had behavior concerns, but again he was slow with his work and he often did not complete assignments. She felt he was often tired.
According to the teacher, he disliked PE class, but he seemed to enjoy music and art class and he liked science. She did say he liked math too but sometimes he had a hard time copying the math problems from the board and getting his math finished. So, even though he was good at mental math, the copying of the problems was very difficult for him. Figure 5 shows the assessment results.
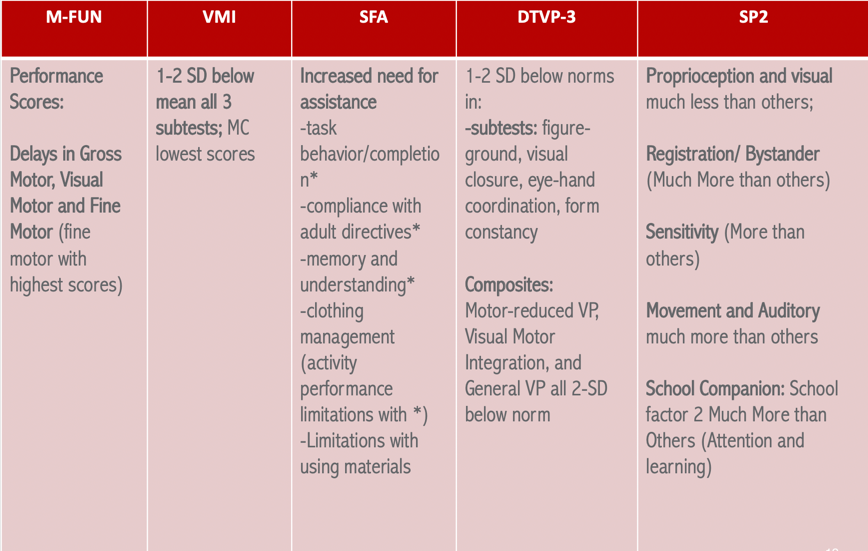
Figure 5. Assessment results.
The M-FUN results are not surprising because we knew he had some motor issues. Gross motor, visual motor and fine motor all came back as delayed. However, his fine motor had higher scores which means that they were not quite as involved as his gross motor and the visual motor functioning. On the VMI, he scored one to two standard deviations below the mean on all three subtests. However, motor coordination had the lowest scores, and that is the activity where you connect the dots. This makes sense as this one requires some motor control. I started to get a hypothesis as he was lacking the control for this subtest and that score was lower than the drawing one. I began to wonder about his oculomotor skills. The SFA said that he had an increased need for assistance on-task behavior and compliance with adult directives. These results are very similar to the teacher's report. He also had issues with memory and understanding, and clothing management. From the DTVP-3, which measures figure-ground visual closure, eye-hand coordination, form constancy, and all those visual perceptual things, he was below the norm by one to two standard deviations. He was also two standard deviations below the norm for motor-reduced VP, visual-motor integration, and general visual perception. What you are beginning to see is that it does not really make a difference if there is a motor component involved (like using a pencil to follow a track) or just using his eyes. This is a red flag that there is something going on at those lower hierarchal levels of development with respect to ocular motor functioning as well as attention. Finally, Sensory Profile 2 (SP2) showed that proprioception and visual were much less than others. He was showing low registration for those, but he also had sensitivity more than others. He also showed much more registration/bystander tendencies. And then for movement and auditory areas, these were much more than others. We are starting to see a picture here of vestibular challenges, proprioceptive challenges, visual challenges, and attention and learning using the SPSC (Sensory Profile School Companion). These results support that he was most likely missing some of those lower-level skills.
When I did the screening to test this by asking him to track and scan and tested functional saccades, I do not think it will be a surprise to tell you that this was all difficult for him. Saccades were really the area of dysfunction as well as cognitive loading with smooth pursuit. To assess cognitive loading was smooth pursuits, you have them follow an object in nice smooth patterns about 10 inches from their face. Then, you start asking them very basic questions that are long term memory kinds of things like, what did you like for breakfast? Or, who is your favorite TV character? What is your dog's name? If you see a huge discrepancy between their smooth pursuits and the cognitive loading, you will then know that there are some significant oculomotor control issues, and they are going to affect school performance. All of this information aligns with not only things we heard from school but also concerns the mom had as well.
Assessment Research
I wanted to give you just a little bit of information from the research on assessments so that this can inform your clinical reasoning (see Figure 6). Some of this is older but it is quite interesting.
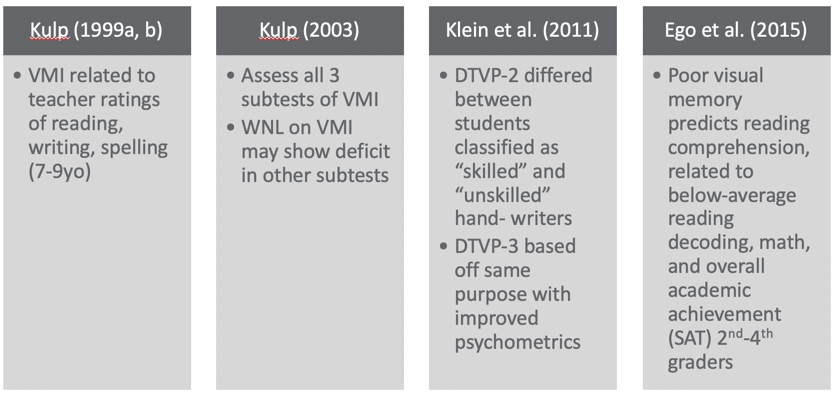
Figure 6. Overview of assessments.
The VMI is commonly used, and it is cheap and easy. In this study by Kulp (1999), it was related to teachers' ratings of reading, writing, and spelling. I think a lot of people use VMI for handwriting. It is not an effective tool to identify handwriting issues, but rather it is more effective at showing us writing, reading, and spelling challenges for ages seven to nine. This is why I chose it for Patrick. Another study, by Kulp (2003), showed that all three subtests of the VMI are really important instead of just doing one. This is because you might get "within normal limits" on one, but you might get that result on another one. For example, the blue subtest focuses on visual discrimination and if they can match a picture. Thus, it does not really give you a lot of information on other areas. Thus, Kulp recommends doing all three subtests. This is very interesting about the DTVP-2 in a study by Klein et al. (2011). The results actually differed between students classified as skilled and unskilled hand writers. So, if you want to look for handwriting challenges and figure out where the difficulties are coming from, the DTVP-3, the new version, is based on the same purpose as it just has better psychometrics. They tightened up the validity of the reliability scores in the newer version. Lastly, poor visual memory predicts reading comprehension (Ego et al., 2015). Kids who have poor visual memory also will have below-average reading, poor math decoding, and academic achievement scores for second to fourth graders. Visual memory becomes very important for this age group if they are struggling in school. This is why I use the DTVP. The TVPS (Test of Visual Perceptual Skills) is okay too but it does not capture the composite of motor versus non-motor.
EBP Remediation: Skeffington’s Model
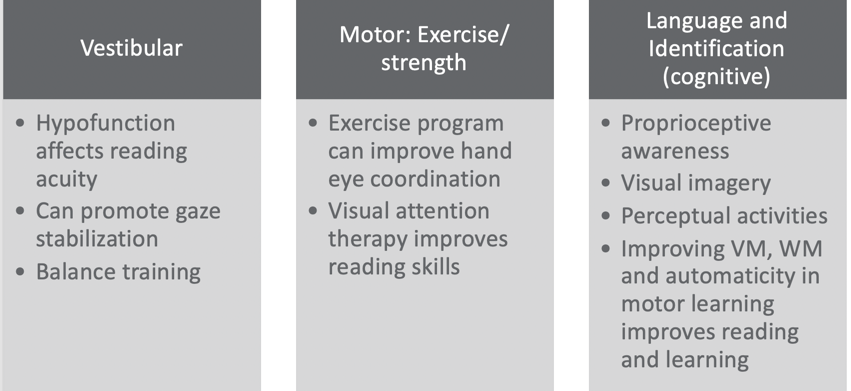
Figure 7. EBP remediation using Skeffington's Model. (Christy, 2019; Shelly-Tremblay et al., 2012; Gibson et al., 2015; Garje Mona et al. 2015; Jamal et al. 2019; Grisham et al., 2007; Sweeney et al., 2014; Mast et al., 2014, Gaymard et al., 2017; Van Hecke et al., 2019.)
Using a Skeffington's Model approach (see Figure 7), if we look at the vestibular function of Patrick, we start to realize that if you have an under-responsive vestibular system, it can affect reading acuity. Vestibular promotes gaze stabilization and balanced training related to your vestibular function for vision. He actually seemed to have a hypo functioning vestibular system according to the SP2; however, he had some over responsiveness when you looked at his post-rotary nystagmus. For the centering or motor area, exercise programs can improve hand-eye coordination. From multiple studies, the reasoning is that as the kids start to have better posture, strength, and endurance, they begin to be more aware of their bodies. Body scheme or kinesthetic awareness can also improve. They also found that visual attention therapy improves reading skills, and that visual attention therapy could result from exercise and strength programs. We also know that if someone can sustain sitting upright for a while and has postural control, they also will have better cognitive attention. However, visual attention really relies more on staying upright and sustaining a gaze on something, then there will be improved visual attention. It makes sense that if I have more postural strength and dissociation, I can do that.
Then, I combined language and identification together as the cognitive components of vision. What is very cool about this one is that proprioceptive awareness becomes very important per the research. The more proprioceptively aware you are, the higher the level of visual perceptual skills. They seem to correlate. Visual imagery became extremely important within this. You have to have some visual imagery and that involves the retina. The vestibular system interacts with the visual system as well as the proprioceptive system to provide stability within your environment. As we negotiate, through our activities, it allows for an image to be obtained by the retina and this happens as you are also moving your head to access things. Your body then integrates it. It starts to get really complicated very quickly. If I put all these things together, I start to become someone who has this dynamic ability to hone in on something, look at it, get that retinal involvement, and then start that whole processing procedure. We need the whole body in order to see. Studies also show that perceptual activities become extremely important. And if you improve visual memory (VM) and working memory (WM), as well as automaticity in motor learning, you will see improved reading and learning. This one I think really speaks to us as OTs. We might not necessarily think that that correlates to reading and learning skills, but it really does fit in this language and identification piece. If you think about it, with visual memory you now have a bank of things from which to pull, and then you can start moving up the hierarchal ladder. Working memory is being able to utilize your functional memory at the moment, and that does require visual memory as well as auditory memory. Automaticity is saying that my motor learning ability has moved beyond the skill level, and I am not in the cognitive learning level of motor learning. I have moved into the third level of motor learning which is that autonomous level where I can do something without really making a lot of errors and having to think about it. If we can get a child to the autonomous level, we will see that reading and learning flourish. This is really focusing on handwriting for the most part because that is often the tool that we use (written communication in our school occupations). If a child is focused on writing, it is really going to be hard for them to do anything else. And, when we are stuck in the motor learning cognitive phase, it can frustrating, exhausting, and hard. If we can get them beyond that level to where they are more automatic, it is much more functional for learning. A child cannot learn if they are dividing their attention. Figure 8 reinforces what we just talked about.
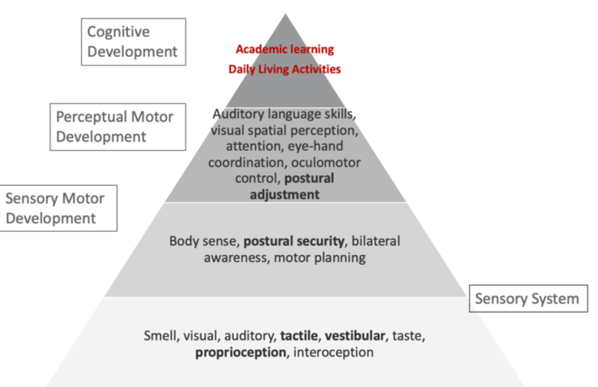
Figure 8. Sensory, motor, and cognitive development (Hk playgroup, n.d.).
The bottom part of this triangle is the very basic sensory system. The next one is the sensory-motor development. This includes body sense, postural security, bilateral awareness, and motor planning. This 2nd tier has been informed by the sensory system. Once this is pretty good, you start to develop more perceptual-motor development which is auditory language skills, visual-spatial skills, eye-hand coordination, oculomotor control, and postural adjustment. You start to see how this developmental pattern starts to make sense with vision and cognition. The top tier is academic learning, daily living activities, and the occupations that we focus on. They need a lot of these underlying skills to be able to do it. The foundation or the sensory piece is so important to vision, but all of these sensory pieces inform our subjective processing of visual information.
Remediation Approaches
Let's now see some of the remediation approaches that were used with Patrick (see Figure 9).
Motor
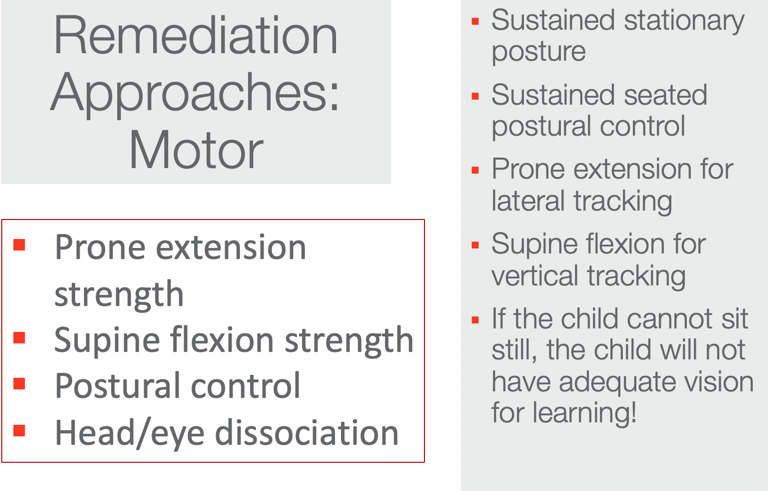
Figure 9. Motor approaches.
If I am going to treat oculomotor skills to try to build visual attention, I need to focus on postural strength, endurance, postural control, and head eye association. Now, all of a sudden, they become little visual receptors. They can receive information while moving within their environment. What does that look like in therapy? These can be all sorts of cool activities that really work on improving that strength like yoga and crawling around doing things to get stronger. It is important to have this postural strength and control for tracking and adequate vision for learning. I want to explain to you a little bit more about prone extension and supine flexion. I want you to take your fingers and put them on the back of your neck. In the middle of your neck, lightly palpate while your eyes are tracking laterally or horizontally. I want you to feel what is happening in the back of your neck as you are scanning. You should feel a contraction. There is a direct relationship between your lateral or horizontal tracking and your posterior or extensor neck muscles. This is the same if you go into the front of your neck. This is a little trickier to find. Lightly palpate the front of your neck during vertical tracking, and you should also feel a very slight contraction. These areas can facilitate improved tracking if you can strengthen them.
Vestibular
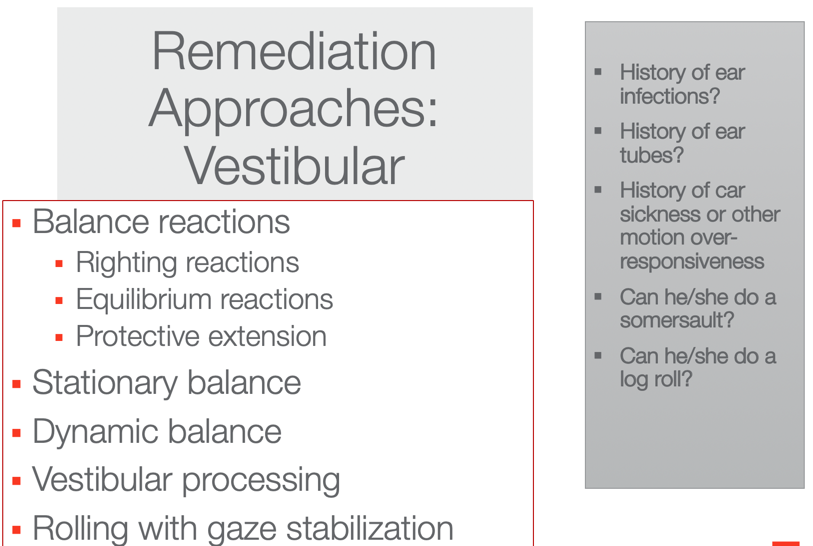
Figure 10. Vestibular approaches.
We want to determine a history of ear infections, ear tubes, or car sickness. Can they somersault? Can they log roll? These can tell us how their vestibular system is working. And, these are activities that we want to work on with these kids to really get that antigravity circle of Skeffington's Model working. I also want to make sure that their balance reactions are working. I like to use an onion swing for this kind of thing. Another activity is rolling with gaze stabilization. When they are ready and are not getting nauseous from these movements, we can have them log roll or somersault forward or backward and then have them stop and practice gaze stabilization on something. Then, we can have them roll again, stop, focus their gaze, and so on. There are a million ways to do it that can be fun. With these types of approaches, you are going to see a huge change in the function of the saccades.
Case Application: Patrick
- Perform top-down occupational analysis and find a discrepancy
- Identify and incorporate occupation-based practice to address discrepancies
- Final occupation-based activity mimics real activity in context
- Incorporate adaptations as needed (including education and consulting)
- Embed vestibular, motor, and cognitive-perceptual based upon visual hierarchy and discrepancies
Let's apply a top-down approach to our friend Patrick. During this top-down occupational analysis, we want to incorporate occupation-based practice to address those discrepancies as we do not function without occupation. Thus, the final occupation-based activity should mimic a real activity in context. We want to incorporate adaptations as needed including educating the parents and the teachers. We also want to embed vestibular, antigravity, motor, centering and cognitive-perceptual activities. This is where it can get a little tricky. What I want you to appreciate here is that if you see a deficit, like pattern recognition, you treat one level below. You do not start at the level of dysfunction in the hierarchal development, but you always start one level below.
If I find that Patrick's issue is at the lowest level, there really is not anything lower to go so that is where we are going to start. I would send them to optometry anyway to make sure visual acuity is okay. If I had a kid whose issue was visual memory and that was the deficit that really stuck out to me on whatever assessments I did, I would start with pattern recognition. Again, it is important to go one level below.
Figure 11 shows this top-down approach that I was just talking about.
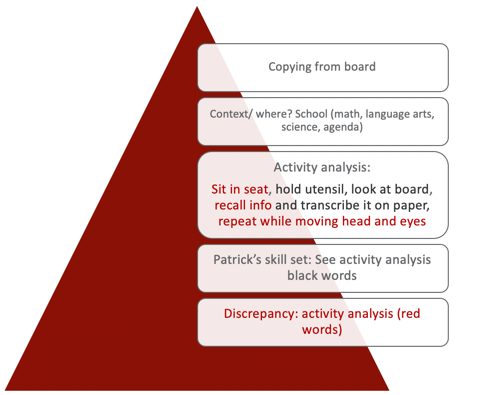
Figure 11. Top-down analysis 1.
If the goal if for Patrick to copy from the board, we want Patrick to be able to copy from the board. In his class, he had to copy a journal topic, math problems, and spelling words from the board. I could have gotten a little more focused on this pyramid, but I kept it general. What is the context? Where does it happen? This activity happens in school during math, language arts, science, and also his agenda. The next thing we would do is an activity analysis. As OTs, this is our special sauce. This is what makes us really unique. I realized this the more I do presentations to other disciplines. We really know how to do an activity or occupational analysis. I did a very basic one here but he has to sit in his seat, hold the utensil, look at the board, recall the information, transcribe it on the paper, and then repeat that as he moves his head and eyes until he gets everything copied. The next level of the process is looking at Patrick's skill set. Those are the black words in the activity analysis. He could hold the utensil, he could look at the board, and he could transcribe it. If this is true, what is the discrepancy between the activity analysis and Patrick's skills? This information is the red text. Sitting in the seat, recalling the information, and then repeating it over and over while moving his head and eyes was difficult for him. Right away that tells me that he has difficulty with centering, vestibular function, and probably something to do with the language like the recalling or identification of the information. I suspect this is because he has difficulty with proprioception. The focus of my treatment then is getting towards a sustained posture, working on the association of head and eyes with gaze stabilization, and visual memory. Activities that I could do in our therapy sessions would be things like Mad Libs. Some of you might have done these as kids. I love Mad Libs and the kids really enjoy them. Secret decoding is another fun one. Other activities I use are scavenger hunts and obstacle courses. I can then embed the things that I need a child to work on like vestibular gaze stabilization and postural strengthening. We used to do something called "Patrick Olympics" which was where we would just come up with different activities. I would pick some and he would pick some. He would try to do all of the activities to get a gold medal. Here's another one in Figure 12.
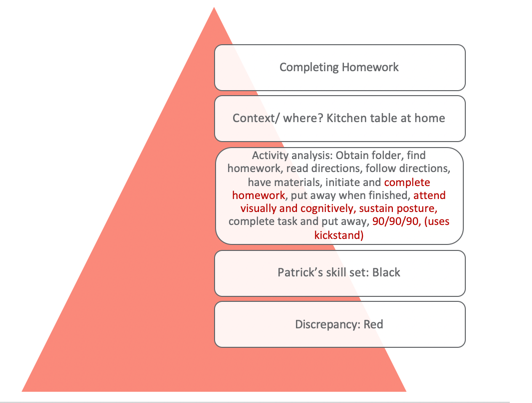
Figure 12. Top-down analysis 2.
This one is for completing homework. You can see in the activity analysis the different steps involved. Again, Patrick's skills are the ones that are in black and then the discrepancies are those in red. Our focus is going to be completing the task which requires sustained attention, postural and bilateral integration, and environmental supports, which I am going to get to in a second. Activities we used included Mad Libs and fantasy football. For the fantasy football activity, we had to come up with something that would be similar to completing a homework assignment. I made it second grade appropriate but it had football charts and plays as he is really into that. He loved that because he got to draw up these little football charts and he got to teach them to me. The goal was that he had to finish the assignment. He also loved to mimic a fireman so I had him "stop, drop and roll" through an obstacle course. This tapped into his vestibular system. Figure 13 looks at buttoning and zipping his pants.
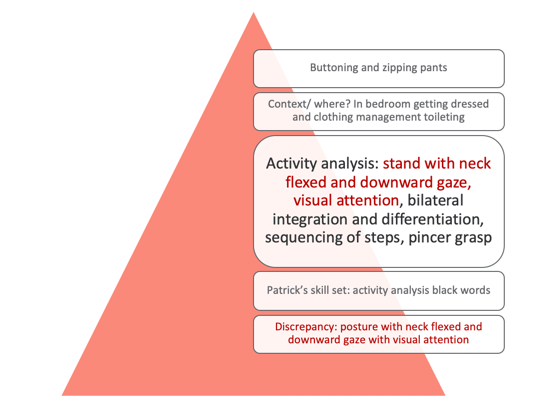
Figure 13. Top-down analysis 3.
Again, you can see in the activity analysis that his skill set is in black and the discrepancies are in red. With this one, I am focusing on his posture with sustained neck flexion and downward gaze with sustained visual attention. This can be a very hard task for kids. For occupations, we did mini golf which was great for this posture. We also did an egg game. The egg game is where you have to carry an egg in a little pouch. While you are walking, you have to watch the egg with a downward gaze and go very slow or the egg will fall out. If it breaks, you lose. It is silly but kids love it. Crab soccer is another great one as it facilitates that neck flexion in sustained pattern. We also did a game called fire rescue. This was done on a scooter board in supine. He had to find "fires" throughout the environment, and he had to keep his neck in a flexed position. Again, it is important to embed some of these activities that align with the Skeffington model approach.
Evidence-Based Approaches: Adaptive Approaches
Figure 14 shows some adaptive approaches.
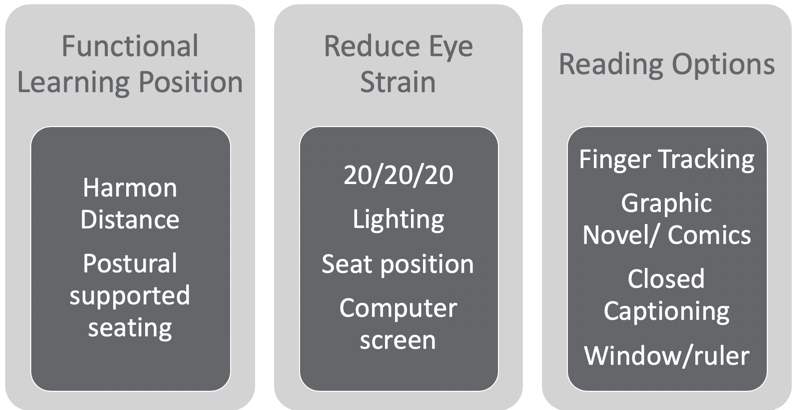
Figure 14. Adaptive approaches.
The functional learning position is really important and this is called the Harmon distance. The Harmon distance is the distance from your fist resting on your cheek to your elbow. This is an evidence-based approach for maximizing visual learning. We also need to look at postural supported seating. If somebody is struggling, we want to make sure that they are supported. This is not news to any of you but really making sure that the desk and the table fit the kid. You know that in the school system or even at home, that is not always the case.
Another approach is to reduce eye strain. A great tip is the 20/20/20 rule. Every 20 minutes, you stare at an object 20 feet away for 20 seconds to recalibrate your eyes and relax the tension. You also want to make sure the lighting is good, and fluorescent lights are not ideal. Again, the seated position is important. We want to make sure that they are not somewhere where they constantly have to strain. For computer use, they really should take a break every 20 minutes from the computer screen. And, if you can get them on a black background with a white font instead of white with black, it's better. The other thing with reading on the computer is that there is no point of reference. For example, on a post-it note or piece of paper, there are four corners of orientation. If I turn it to the backside, again, there are four corners of orientation. There is a sequence to how you read with the boundaries. This does not happen when you are reading a book on a Kindle or on a computer. You lose those corners of orientation. You and I know how to read so we do not need those corners of orientation as our skills are already intact. However, kids are still learning and gaining skills. They need those corners of orientation for reading comprehension, sequencing of events, and trying to find things. It really sort of happens in a vacuum when you are in a Kindle or an online book. Some of you might have even experienced that when you are unable to find a passage or page. Researchers are starting to find that reading online is not good for learning to read or for school development.

Figure 15. Adaptive approaches.
If kids use their fingers to read, let them. It helps them so do not take that approach away. Graphic novels and comics are fantastic. They give them a visual supplement to the reading, and the text is usually not as dense. Closed captioning is probably one of the best ways to help. You can have them watch videos and have the closed captioning at the bottom. This has been shown to cause parts of the brain for reading to light up in a functional MRI. That also works really well for kids with dyslexia. I also like using the window method or a ruler to help with reading. This can be used to block out whatever is below and helps them to focus.
Patrick tends to use a kickstand, or his arm to support his head. Can we set up his desk to achieve the Harmon distance (see Figure 15) and give him proper support? We already know that Patrick is using his finger so we would want to let him keep doing that. I also think the closed captioning would be great. I could recommend that his mom use closed captioning for tv and movies. I could also investigate if he would like to read graphic novels or comics.
Resources
- https://www.trianglevisions.com/blog/your-childs-vision-development/
- https://www.aao.org/eye-health/tips-prevention/children-vision-development
- http://www.healthofchildren.com/E-F/Eye-and-Vision-Development.html
- VERA vision screening program https://visualscreening.com/
- https://www.covd.org
- AMAZING blog with lots of sections: https://visionhelp.wordpress.com/
Here are some helpful resources. VERA is a free vision screening program, and they invite occupational therapists to join in. It is awesome, and I highly recommend you check it out. I also love the VisionHelp blog on the bottom. There are a bunch of sections to help you learn some in-depth stuff about vision. The developmental optometrist on there is amazing, and he explains everything. COVD is a group of vision folks that come together so that is a good one as well.
References
Alenizi, M. A. K. (2019). Effectiveness of a program based on a multi-sensory strategy in developing visual perception of primary school learners with learning disabilities: A contextual study of Arabic learners. International Journal of Educational Psychology, 8(1), 72-104.
Bense, M. S. (2016). The effect of an oculomotor-vestibular-proprioceptive sensory stimulation programme on reading skills in children aged 8 to 12 years 11 months (Doctoral dissertation).
Chokron, S., & Dutton, G. N. (2016). Impact of cerebral visual impairments on motor skills: implications for developmental coordination disorders. Frontiers in psychology, 7, 1471.
Christy, J. (2019). Use of vestibular rehabilitation in the pediatric population. Perspectives of the ASHA Special Interest Groups, 4(6), 1399-1405.
Cohen, D., & Xavier, J. (2017). Oculomotor impairments in developmental dyspraxia. The Cerebellum, 16(2), 411-420.
Ego, A., Lidzba, K., Brovedani, P., Belmonti, V., Gonzalez‐Monge, S., Boudia, B., ... & Cans, C. (2015). Visual–perceptual impairment in children with cerebral palsy: A systematic review. Developmental Medicine & Child Neurology, 57, 46-51.
Garje Mona, P., Dhadwad, V., Yeradkar, M. R., Adhikari, A., & Setia, M. (2015). Study of visual perceptual problems in children with a learning disability. Indian Journal of Basic and Applied Medical Research, 4(3), 492-97.
Gaymard, B., Giannitelli, M., Challes, G., Rivaud-Péchoux, S., Bonnot, O., Cohen, D., & Xavier, J. (2017). Oculomotor impairments in developmental dyspraxia. The Cerebellum, 16(2), 411-420.
Klein, S., Guiltner, V., Sollereder, P., & Cui, Y. (2011). Relationships between fine-motor, visual-motor, and visual perception scores and handwriting legibility and speed. Physical & Occupational Therapy in Pediatrics, 31(1), 103-114.
Kulp, M. T., & Sortor, J. M. (2003). Clinical value of the Beery visual-motor integration supplemental tests of visual perception and motor coordination. Optometry & Vision Science, 80(4), 312-315.
KULP, M. T., Edwards, K. E., & Mitchell, G. L. (2002). Is visual memory predictive of below-average academic achievement in second through fourth graders? Optometry & Vision Science, 79(7), 431-434.
Jamal, K., Leplaideur, S., Leblanche, F., Raillon, A. M., Honoré, T., & Bonan, I. (2019). The effects of neck muscle vibration on postural orientation and spatial perception: A systematic review. Neurophysiologie Clinique.
Mast, F. W., Preuss, N., Hartmann, M., & Grabherr, L. (2014). Spatial cognition, body representation, and affective processes: The role of vestibular information beyond ocular reflexes and control of posture. Frontiers in integrative neuroscience, 8, 44.
Quaid, P., & Simpson, T. (2013). Association between reading speed, cycloplegic refractive error, and oculomotor function in reading disabled children versus controls. Graefe's Archive for Clinical and Experimental Ophthalmology, 251(1), 169-187.
Sales, R., & Colafêmina, J. F. (2014). The influence of eye movement and the vestibularocular reflex in reading and writing. Revista CEFAC, 16(6).
Solan, H. A., Shelley-Tremblay, J., & Larson, S. (2007). Vestibular function, sensory integration, and balance anomalies: A brief literature review. Optometry and Vision Development, 38(1), 13.
Van Hecke, R., Danneels, M., Dhooge, I., Van Waelvelde, H., Wiersema, J. R., Deconinck, F. J., & Maes, L. (2019). Vestibular function in children with neurodevelopmental disorders: A systematic review. Journal of Autism and Developmental Disorders, 1-23.
Citation
Quint, N. (2020). Pediatric case study: Child with oculomotor and perceptual challenges. OccupationalTherapy.com, Article 5120. Retrieved from http://OccupationalTherapy.com
