Attention Deficit Hyperactivity Disorder (ADHD)
Hello everyone. Today, we are going to be talking about attention deficit hyperactivity disorder. I consider this to be under the umbrella of "invisible diagnoses." This population has a special place in my heart because it is very easy to misconstrue some of the challenges that they have as intentional and behavior-based, and therefore, sometimes they get a bad rap. Thus, I am always happy to help kids with ADHD.
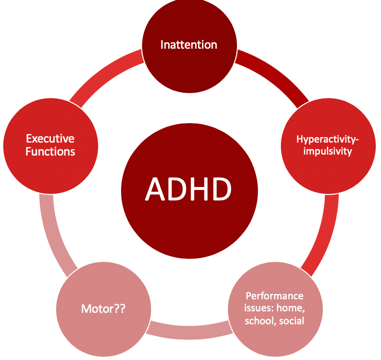
Figure 1. Overview of ADHD.
Individuals with ADHD have a lot of challenges that affect their occupational participation and performance. I think most of us are very comfortable with the idea that inattention, hyperactivity, and impulsivity are the hallmarks, but what sometimes can get lost is the idea that executive functions are very much affected by impulsivity. Motor issues are also often involved with kids with ADHD and are not always considered. In fact, there is a lot of evidence to support that the motor needs of these kids often go unaddressed. Typically, these kids come to us when parents or schools have major concerns about their behavior. Therefore, this tends to be where everyone focuses their attention. Oftentimes, the motor issues then fly under the radar and do not get addressed. The cool thing is that motor interventions can be the means to make some really significant changes for these kids, particularly in the area of executive function. There is a win-win situation when we address the motor issues. Lastly, they tend to also have performance issues not only in their home environment but also in their school and social environments as well.
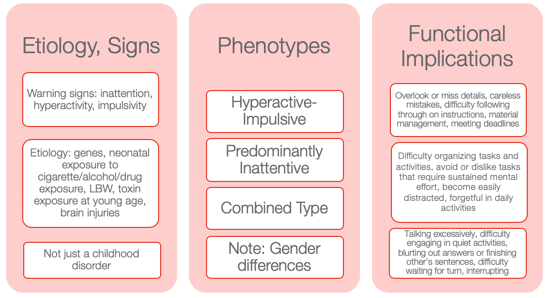
Figure 2. Other information from the NIMH Information Resource Center (2020).
I wanted to provide some information to help you to appreciate how diverse ADHD is. Many might still use ADD when we are talking about the children who have an inattentive type as it seems to make more sense. However, that is not how it is defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM–5).
Etiology and Signs
The etiology and the signs are inattention, hyperactivity, and impulsivity. We also know there is a genetic predisposition to this. Neonatal exposure to cigarettes, alcohol, and drugs can also lead to ADHD. Low birth weight and toxin exposure are some of the environmental elements. ADHD can also be the result of a brain injury. This is not just a childhood disorder, and people do not grow out of it. In fact, the symptoms can actually get worse as life gets harder as one gets older. Adults who have ADHD can have some significant struggles, particularly if they do not know that they have ADHD or if it was never addressed.
Phenotypes
There are three phenotypes: hyperactive-impulsive type, predominantly inattentive type, and a combination type. I think the hyperactive-impulsive type is the picture most people have when they think of ADHD. Then, we have the predominantly inattentive type. These are the daydreamers or the individuals that jump from one thought to the next. They have a really hard time staying focused for long. Lastly, there is the combined type. This is where we see both elements of inattention and hyperactivity and/or impulsivity. I think it is really important to also appreciate gender differences. You can see very different types of ADHD in girls versus boys. Boys obviously tend to be of the hyperactive-impulsive type, but even the inattentive type can be a little different. Girls, who have ADHD, tend to be talkative and a little more anxious. They definitely have a different predisposition as opposed to the boys. Thus, it might be the same diagnosis but look very different between the genders.
Functional Implications
Functional implications become extremely important. These are individuals who tend to overlook or miss details. They might make careless mistakes. They have difficulty following through with directions at school. Material management can become very challenging especially dealing with paperwork. They can miss deadlines and have a hard time keeping track of and prioritizing tasks. These are some of the higher-level executive functions. You might also see an avoidance or an expressed dislike of tasks that require a significant amount of sustained mental effort. They might tell you it is too hard, and they might feel very overwhelmed. They become very easily distracted by anything. The use of electronics adds to the issue. They can be forgetful in daily activities, talk excessively, have difficulty engaging in quiet activities, and tend to blurt out answers or finish others' sentences. Often, the perception is they are interrupting and being rude. They may have difficulty waiting for their turn or interrupt during someone else's turn. These are examples of impulsive behaviors. We will talk more about this when we get to executive functions.
Differential Diagnosis Between ADHD and SPD
- A high rate of comorbidity between SMD and ADHD
- ADHD and SMD
- Both at risk for limited participation in many aspects of daily life
- ADHD slightly worse attention scores than SMD
- SMD
- Tactile, taste/smell, and movement sensitivity, visual-auditory sensitivity; behavioral manifestations of sensory systems
- Exaggerated electrodermal responses to sensory stimulation, thus increased risk of sympathetic “fight or flight” reactions
(Miller et al., 2012; Yochman et al., 2013)
Sometimes, kids who have ADHD also have some sensory issues. You may wonder, "Do they have just ADHD by itself?" This is probably one of the most common questions I get when working with kids with ADHD whether it is from teachers, other therapists, or from parents. Next, we are going to be talking about a child who has straight ADHD. However, for a few minutes, I want to talk about the whole idea of differential diagnosis between ADHD and SPD and how this all fits together. There is a very high comorbidity between sensory modulation disorder and ADHD. When I am referring to sensory modulation disorder, I am using the Lucy Jane Miller nosology. Sensory modulation disorder refers to the over-responsive, under-responsive, and/or craving of sensory input. For both ADHD and sensory modulation disorder, you will see that these diagnoses are both at risk for limited participation. These are kids who will not participate in certain activities because the sensory input is too much or overwhelming for them. ADHD will have slightly worse attention scores than SMD when you complete a formal attention test like the Test of Everyday Attention. However, you will see the same kind of impulsive behaviors.
Those with sensory modulation disorders tend to have difficulty with tactile, taste, smell, and movement sensitivities. You might also see some visual-auditory sensitivity so there are some behavioral manifestations that come of that. They might become stressed related to fears of vestibular or other movement input. They might also dislike certain noises or touch.
They found in the research that sensory modulation dysfunction, not ADHD, will have an exaggerated electrodermal response to sensory stimulation. This means that they have an increased risk of sympathetic activation which is the fight-or-flight, freeze/faint reactions, and meltdowns. When you have a child with meltdowns, you want to investigate if they have sensory modulation dysfunction right away. And, if you have a child with ADHD who does not have a history of meltdowns, that is a really good sign of your initial hypothesis. While this alone does not mean that they do not a sensory modulation dysfunction, chances are that they do not. Additionally, they might have dyspraxia or a discrimination disorder.
This is just a brief summary of how this all comes to play with an ADHD diagnosis and possible comorbidities.
Case Introduction: Jeremy (Age 9, ADHD, Combined Type)
- He lives with his mother and older sister in SFH and goes to his father’s house on the weekend (divorced)
- He is in the 4th grade and has an IEP for OHI
- Strengths: funny, good at math, helps the family to take care of pets, watches WWE with father, loves dogs, likes to play board games (Monopoly, Sorry)
- School concerns: material management, organization, completing tasks or losing work, impulsive, social difficulties (short-lived relationships, fights), “lacks self-control” and “messy”, underperforming and sometimes seems “lost”
- Family concerns: Fights with a sibling, sleep difficulties, messy room, messy notebooks, and backpack, loses things, avoids homework, resists bedtime, difficult to wake in the morning and slow with routine, poor hygiene
- Jeremy’s goal: make friends, be able to find his schoolwork, have good friends, be better at kickball and wrestling
Jeremy is nine, and his diagnosis is ADHD, combined type. I have a feeling Jeremy is probably similar to a lot of the kids you see. I know I have seen a lot of these types of kids. He lives with his mother and older sister in a single-family home and goes to his father's house on the weekend because of a divorce. He is in the fourth grade, is eligible for an IEP because of an OHI (other health impairment), and is eligible for special education services because of his diagnosis of ADHD.
I always like to start with strengths with all kids, especially ADHD because these kids can have a really hard time with confidence and self-esteem. They also get blamed for their behaviors. For his strengths, he is funny, good at math, and he likes to help take care of his pets at home. He likes to watch wrestling, World Wrestling Federation (WWF) with his father, loves dogs, and loves to play board games. He is really good at Monopoly and Sorry.
At school, he had challenges with material management, organization, completing tasks, and not losing work. These last two are highlighted as we are going to focus on that. He is impulsive, and he has social difficulties. His teacher described his relationships as short-lived. He would have a friend, and then all of a sudden, they were not friends anymore. She also reported that he lacked self-control, was messy, and thought he underperformed. And, she felt like he always seemed lost. When they were going through the instructions or going through something, he was always looking at his peer's work or looking confused while he was trying to figure out what was going on.
The family had some concerns about his fighting with a sibling, significant sleep difficulties, a messy room, messy notebooks and backpack, and that he would often lose things. He also avoided his homework and resisted bedtime. As a result, it was very difficult to wake him up in the morning, and he was slow with his AM routine. His mom said that he also had an impulsive way of performing hygiene tasks. For example, he would brush his teeth in two seconds and say he was done. Everything was quick and impulsive. This is very typical for boys with this type of ADHD.
His goals were to make friends and find his school work. He said it was very stressful to always feel like he was losing his school work. He was motivated to do well in school. He did not just want to make friends, but he wanted to have good friends. He also wanted to be better at kickball because that is what the kids played at recess and in PE. He also wanted to be better at wrestling as not only did he like to watch with his dad, but he also liked to wrestle with him.
I want to go back to the highlighted areas in my list: completing tasks, losing work, and difficulty waking in the morning. These are the areas we are going to focus on.
Assessments
Assessments are one of the most challenging things for people because they are often under a time crunch, and the reports are difficult to write up and are time-consuming. However, it is really important with these kids as it gives us a full perspective on where they are having challenges. Knowing that he has "ADHD combined type" does not really tell us about his occupational performance and participation. We want to really get all that information. I like to be pretty thorough, and I will scatter assessments throughout my time with them to try to get a good idea. Again, I really like to check out their motor skills. I have kids that are superstars in sports, but I will still find out that there are some motor problems.
Typically, the motor challenges with ADHD have to do with bilateral coordination, dexterity, and those kinds of things. They might be good at some things, like basketball or baseball, but this does not mean that they are good at fine manipulation. Thus, it is really important to find out where they are. Figure 3 shows a summary of the assessments I did with Jeremy.
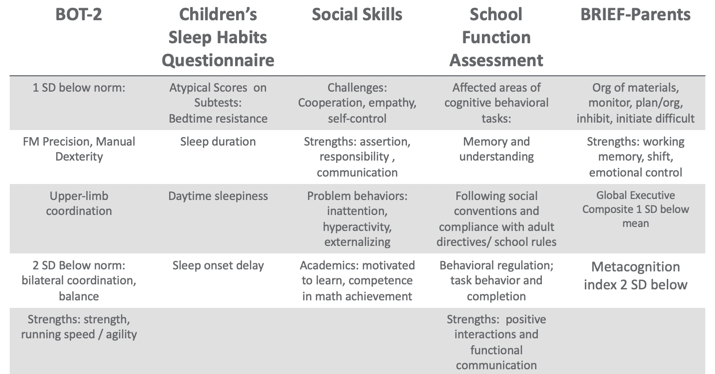
Figure 3. Assessment results.
Using the BOT, I found that Jeremy was one standard deviation below the norm in fine motor, precision, and manual dexterity, which was not surprising. He was two standard deviations below the norm in bilateral coordination and balance. However, his overall strength, running speed, and agility were fine.
There are many great tools out there for sleep including free ones. One of my favorites is the Sleep Habits Questionnaire. It is free online. It is great because it uncovers behaviors regarding going to bed, sleep duration, daytime sleepiness, and sleep onset delay. Many kids with ADHD have an overactive thinking process which then causes a sleep latency problem. It is hard for them to settle their brain and get to sleep. They also might have difficulty with sleep duration and not get enough sleep or good quality of sleep. If their arousal level is still high at night, it' is hard to get them to calm down and want to go to bed, especially if they are very disorganized in their thinking. This questionnaire gives you good information. Our results with Jeremy found that had bedtime resistance, sleep duration, daytime sleepiness, and sleep onset delays that were all atypical scores.
I also did a social skills assessment with him because his goal was to make friends, and school indicated that he had a hard time with solid friendships. I like to have a social-emotional learning perspective, and the more I know about a child's emotional intelligence, the better. We want these kids to be successful in their social interactions because that affects their whole life. With the Social Skills Improvement System (SSIS) Rating Scales, I found challenges with cooperation, empathy, and self-control. His strengths included assertion, responsibility, and communication. Under "problem behaviors", I found inattention, hyperactivity, and some externalizing behaviors. With his diagnosis, this all seems to fit. For academics, he was motivated to learn and had competence in math achievement. We already knew he had strengths in math.
I also did the School Function Assessment. I love this tool. There is one section that is a little dated as it talks about a floppy disk or something, but the other information on there is fantastic. This is especially true if you have kids who have a hard time following rules, social conventions, and material management. You can give it to the teacher, and they can score that. I found that Jeremy had some affected areas with memory and understanding, following social conventions, and compliance with adult directives and school rules. Additionally, he had some behavioral regulation issues, and task behavior and completion were difficult for him. His strengths included positive interactions and functional communication. Communication is strong for him,= which is a good thing.
The BRIEF (Behavior Rating Inventory of Executive Function) is an executive function tool that I did that with his parents. What we found was that the organization of materials, monitoring, planning and organization, inhibition, and initiation were difficult for him. His strengths were his working memory. Additionally, cognitive shifting and emotional control were also strong. However, his global executive composite was one standard deviation below the mean which means that he was low in everything. While it was not devastatingly low, he was below the average in everything. He struggled the most in metacognition, and that was two standard deviations below the norm. Thinking about his own thinking was a struggle for him.
From an observation standpoint, I also got a video from him mom of his AM routine so I could see what that looked like. He was in slow motion, very tired, not wanting to do the routine, and his performance was of low quality, I would put it, writing examples from school, because sometimes you'll see that the handwriting is indicative kind of the brain and the body not matching up, the brain going a little faster than the body. And so I also had a homework video watching him kind of resist homework. And then I did ocular motor testing, checked his tracking, convergence, divergence, and saccades and those kinds of things. Because there is a correlation between having some difficulties with that sometimes. But he actually was fine, and that wasn't a complaint from parents. So I just wanted to make sure it wasn't an issue that we were missing. So that gave me a lot of information.
Research Implications: Assessment
This is information about some of the research implications regarding the assessment process and kind of why I chose the tools that I chose and why I recommend a comprehensive one.
- Motor: Children with parent-reported motor issues received more PT than those with teacher-reported motor issues (risk)/undertreated motor problems in children with ADHD (due to behavioral factors in referral); HW difficulties; higher ADHD and lower motor proficiency scores reported more sleep problems (Papadopoulos et al., 2018)
- Sleep: Sleep deficits negatively affect inhibitory control (Cremone-Caira et al., 2019); Difficulties initiating and maintaining sleep 25-50% in ADHD (Corkum et al., 1998); Prevalence of sleep disorders 84.8 % affecting QoL (Yurumez & Gunay Kilic, 2013)
- EF: Motor skills and EF related (Pan et al., 2015); boys with ADHD have lower EF abilities than typical peers on both performance-based and parent report tools, thus combo is recommended (Sgunibu et al., 2012)
- Social: Children with ADHD 50% lower odds of sports participation than children with asthma with higher incidences of screen time (Tanden et al., 2019); childhood ADHD associated with obesity (Kim et al., 2011); underlying lack of interpersonal empathy (Cordier et al., 2010); Playfulness indicators: ADHD group “typical” with some difficult items but difficulty with basic skills (sharking) (Wilkes-Gillan et al., 2014); seek green outdoor settings at a higher rate (Taylor & Kuo, 2011)
For motor, Papadopoulos and his group (2018) found that there is some difficulty with handwriting. They also reported the higher ADHD and lower motor proficiency scores, the more sleep problems. The fact that Jeremy had sleep problems made me want to look at his motor skills for this reason. This is another interesting one. Children with parent-reported motor issues received more PT than those with teacher-reported motor issues. The fact that we listen to the parents more than the teachers about motor issues is important to consider. Under-treated motor problems in children with ADHD are really due to a behavioral focus so that is why it tends to get missed.
Sleep deficits negatively affect inhibitory control (Cremone-Caira et al., 2019). If we know that these kids have inhibition issues, we need to help them get some sleep. Poor sleep is only reinforcing their challenges and making it worse. They found that there were difficulties initiating and maintaining sleep at a rate of 20 to 50% of kids with ADHD (Corkum et al., 1998). Now, granted, that was 20 years ago, but they have replicated that since. And, if you have a sleep disorder, there is an 84.8% chance that it is negatively affecting your quality of life (Yurumez & Gunay Kilic, 2013).
Motor skills and executive functions are related. If you have some motor difficulties, it is going to influence your executive function ability (Pan et al., 2015). Boys with ADHD have lower executive function ability than typical peers on both performance-based and parent report tools, thus, it is really important that you use a combination of both performance and parent report tools (Sgunibu et al., 2012).
Children with ADHD are 50% less likely to participate in sports than children with asthma (Tanden et al., 2019). I find that amazing. Kids with ADHD also have a higher incidence of screen time usage, and we know that that is always a challenge (Tanden et al., 2019). Childhood ADHD is also associated with obesity. Hence, if you are not doing anything physical and you are sitting there watching your computer or playing video games, and you are impulsive, you are more likely to be obese (Kim et al., 2011). An underlying lack of interpersonal empathy can be something that you often see in ADHD. This affects social abilities and participation and success (Cordier et al., 2010). There are also playfulness indicators. An ADHD group might score as "typical" with some difficult play criteria, but then have more difficulty with basic items (Wilkes-Gillan et al., 2014). Their play may be developmentally out of whack. Again, they might be okay with some high-level types of behaviors, but then when it comes to something simple like taking turns or sharing, they cannot do it. Sometimes we have to go back and practice these rudimentary skills. This might be why they are struggling socially because they are having problems with age-inappropriate items. Lastly, these kids with ADHD really seek green outdoor settings at a higher rate (Taylor & Kuo, 2011). It would be interesting to monitor how outside time might influence their performance on assessments.
EF and Self-Regulation Connection
- 3 Basic Dimensions (Miyake et al., 2000)
- Inhibitory control
- Cognitive/mental flexibility
- Working memory
Can these kids self-regulate? When they cannot, it does not work out well for them in school or at home, and it does not work out well in terms of social abilities. When they become adults, they have trouble keeping and maintaining a job. This is the definition of EF.
Some of you might be very familiar with this definition, but it is also quite complicated. This is how we remember information, filter distractions, resist impulses, and sustain attention during an activity that is also goal-directed. While we also adjust our plan as needed to avoid frustration in the process. That is a lot of working parts. Many times, you see people refer to executive functions like an air traffic controller of information and materials. These are the "big 3."
This is how we remember information, filter distractions, resist impulses, and sustain attention during an activity that is goal-directed while adjusting our plan as necessary and avoiding frustration!
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex "frontal lobe" tasks: A latent variable analysis, Cognitive Psychology, 41, 49-100.
- Inhibition
- Impulse Control
- Requires arbitrary rule be held in mind while inhibiting one response to produce an alternative response (Best & Miller, 2010)
- socially acceptable (Olson, 2010)
- Working Memory
- Ability to store, update and manipulate /process information over short periods of time (Best & Miller, 2010)
- “Limited-capacity information-processing system” (Roman et al., 2015)
- Verbal, visuospatial, and coordinating central executive
- Cognitive Flexibility
- Ability to think flexibly and shift perspective and approaches easily, critical to learning new ideas (different perspectives)
- Requires inhibition and WM processes
- Switching between two or more mental sets with each set containing several tasks rules
- Feedback related (unlike inhibition) (Best & Miller, 2010)
All these things are important, but the three basic dimensions are inhibitory control, which develops first around four years of age, cognitive and mental flexibility, and working memory. Mental flexibility is the result of inhibitory control and working memory working together. If you have a problem with inhibition or working memory, or both, you are going to have problems with cognitive flexibility. The flip side of that would be rigidity. It is also being able to shift your thinking in the moment back and forth. The flip side of that would be to be stuck. Working memory is the ability to use your memory functionally. It is very important to know that we only have a very limited amount of memory capacity, and it is all we have. I like to call my working memory my suitcase. You have to make sure you pack the right things in there for the trip that you are going on. If you pack your suitcase for Fiji and you are going to Alaska, you are going to be on the beach with boots and a parka and be miserable. It is really important that we pull in the information that we need. This takes sustained attention. If you cannot sustain your attention, you are not going to capture the right memories. And again, if there are problems with inhibitory control or impulse control, this is going to be challenging. Impulse control is controlling yourself in the moment. If I can string those together, now I have more self-regulation ability. Again, these are the big three: inhibition, working memory, and cognitive flexibility and shifting.
I already explained these, but I want you to appreciate what the research says. Inhibition requires an arbitrary rule to be held in your mind while you are inhibiting one response to produce an alternative response, which is typically the one that is more socially acceptable. Working memory is storing, updating, and manipulating information over short periods of time. It has a limited capacity, and it is verbal and visuospatial. Then, for cognitive shifting and flexibility, there are two pieces to it. It is being open and being able to shift. Here is what is interesting. Cognitive flexibility and shifting respond really well to internal feedback. You can actually start to observe things and gain some insight and make changes. Why that is important is because inhibition does not get better from internal feedback. It only gets better from external feedback. Think about someone you know who interrupts a lot because they are impulsive. They see that they do it and do not change because no one has said anything to them. It requires external feedback for them to say, "Oh, I'm doing it wrong." We do not have this internal mechanism to change our impulsivity. We cannot assume these kids will figure it out and fix it, because they will not. We have to be very stern and to the point and say, "You're doing it wrong. This is why it's wrong and here's what you need to do instead." This is the key. Figure 4 is an executive function cheat sheet.
(Cooper-Kahn & Dietzel, 2008)
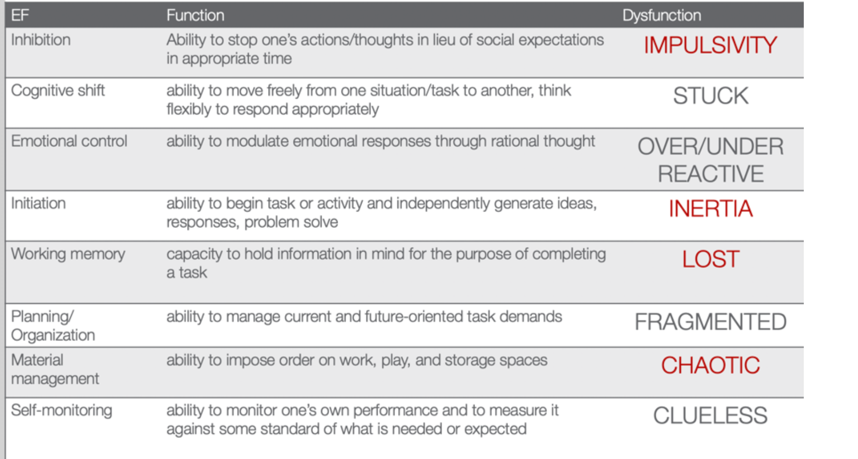
Figure 4. EF cheat sheet.
This is from Cooper-Kahn and Dietzel (2008). They tell you the executive function, what the function is, and then the end dysfunction. For inhibition, the dysfunction is impulsive. If you cannot cognitively shift, you can get stuck. If you do not have emotional control, you are going to be over or under-reactive. If you cannot initiate a task, you are stuck in inertia. If you do not have a good working memory, you are lost. If you cannot plan and organize, you are fragmented. If you cannot manage your materials, you are chaotic. And then, if you cannot self-monitor, you are clueless. The red ones are those that Jeremy struggled with. He was impulsive, had inertia, was lost, and chaotic. He was also a little fragmented and had a difficult time with organization. However, these four things were his biggest challenges.
Review of Evidence-based Interventions for Case
One of the objectives is to talk about evidence and how we are going to use the evidence to support our intervention. I focused on motor, social, executive functions, and sleep. These are the things that were assessed that also had evidence for different intervention strategies (see Figure 5).
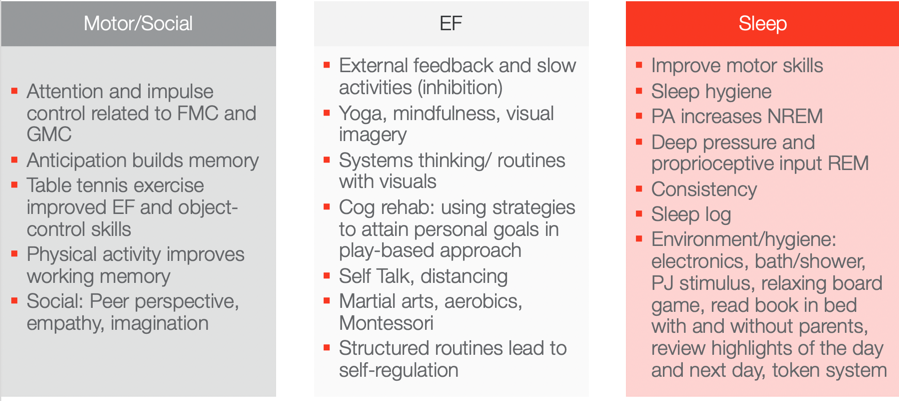
Figure 5. Evidence-based interventions ((Hui Tseng, et al., 2004; Hahn-Markowitz et al., 2016; Washington University, n.d.; Diamond & Lee, 2011; White & Carlson, 2016; Winsler et al., 2009; Marjorek et al., 2004; Kuhn & Floress, 2008; Frike et al, 2006; Keshavarzi et al., 2014).
Motor/Social Categories
Let's look at the motor and social categories. What is really interesting is that attention and impulse control are related to fine motor and gross motor coordination. If we can work on coordination, we can also increase attention and impulse control. This is killing two birds with one stone in Jeremy's case. I do not know who is familiar with Hebbian's law, but it says is that the (brain) cells that fire together wire together. One of the ways to do that is through the concept of anticipation. Anticipation builds memory capacity and will improve working memory. Anticipation is a context, and you can basically put anticipation in anything. With turn-taking, there is anticipation. If there is a competition, there is anticipation among the competitors. If you know you are going to be called on, there is anticipation. If you are playing a game where something might jump out, there is anticipation. These are just a few examples of where you can build in anticipation. If you can add that into your activities, you can build memory capacity. Another study looked at how table tennis exercises improved executive function and object control skills. Table tennis does not require a lot of heavy-duty cardio and it is not a tiring exercise, but it requires a lot of hand-eye coordination and sustained attention. I think this is a really good occupation-based strategy to improve executive function and object control. Physical activity also improves working memory. I have had tons of success with kids doing physical activity both in therapy and at home to improve their working memory. Some of the social strategies that work really for kids, and we will talk about a few in a little bit, is taking a peer's perspective and working on empathy and imagination. These things were really shown to be effective ways to change someone's social success.
Executive Function
For executive function, you have to give them external feedback. You have to tell them when they are being impulsive, and then you have to tell them how to fix it. These are kids who are on a very fast, impulsive temporal context. I talk to them about the hare versus the turtle. I tell them to be more like the turtle. Yoga, mindfulness, and visual imagery are other strategies. Yoga and mindfulness are occupations, and you can incorporate visual imagery into any occupation. They are so effective especially living in a very stressful, fast-paced society. There is self-distancing involved which we know also helps with the social skills for these kids. Systems thinking and routines with visuals are other options. The more visuals we use, the better for these kids. If we can give them visual imagery, it helps. Here is an example of systems thinking. You have family coming over for Thanksgiving dinner. There are 17 people coming and three courses. Each dish takes this long and I need these ingredients for each. Additionally, these dishes all cook at different times so they come out at the right time. This is systems thinking. As a strategy, I gather my recipes and my materials and then put them in order for which ones I have to cook first and for how long. I form a little assembly line of what I am going to do. We can use this type of strategy for kids who struggle with material management and organization. It can be a game-changer. Other ideas include self-talk, martial arts, aerobics, and Montessori. I do not know if anyone has any experience with a Montessori approach. One of the reasons why it is effective is because Montessori uses self-distancing activities. Telling the kids what you want them to do instead of what you do not want them to do really works. It also includes structured routines that lead to self-regulation.
Sleep
The last section shows that motor skills, as well as sleep hygiene, can improve sleep. Physical activity actually increases non-REM sleep. Deep pressure and proprioceptive can increase REM sleep. A sleep log is actually evidence-based as well. Shortly, I am going to describe a routine that works with kids that is evidence-based. All of these things here you can use as your evidence-based toolkit to work with kids with ADHD.
Case Study Application- Improve ADLs
Top-Down Analysis
Jeremy's goal is to have a timely morning routine which involves waking up, dressing, brushing teeth, and packing a backpack. This is a top-down analysis in Figure 6.
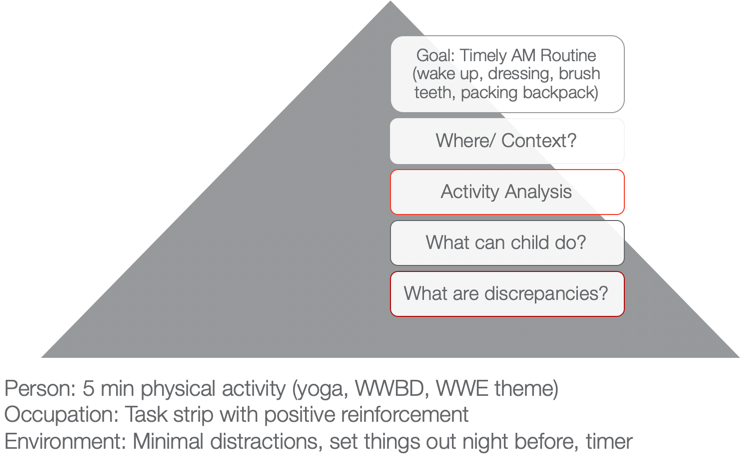
Figure 6. Example of a top-down analysis for ADL routine.
When we use a top-down approach, we are starting with the actual occupation and the goal is to look at where this happens and in what context. I want you to think about where that would happen. In Jeremy's case, it is his bedroom and bathroom. Activity analysis is the bread and butter of OTs. His routine consists of waking up, dressing, brushing his teeth, and packing a backpack. During this analysis, we want to see what he can do and what he cannot do. What are some of your thoughts? Here are some answers from our audience:
- Being aware of time during all tasks/Using a timer. You are seeing a discrepancy between time awareness, time estimation, time monitoring, and time management. I would agree with you that he probably has a hard time all of those.
- Packing the backpack. We know that he is sleepy in the morning and he has a difficult time staying organized. This is especially true if he is half asleep or stressed in the morning.
- Finding his folders. Folders can be elusive sometimes to these kids, so that is a great point. Folders can be found in very strange places.
- Hygiene/organization. Even in hygiene, it is important to make sure that they are organized.
I used a PEO or person-occupation-environment perspective here. We started with some physical activity in the morning to help him to wake up. We did yoga. I asked, "What would Batman do?" He was a big Batman guy. We did some self-distancing by him coming up with strategies for Batman. Or, we used a wresting theme. These activities helped him to be more alert and be able to increase his attention.
We also used a task strip with positive reinforcement to help him see what he needed to do. Visuals can be very helpful for these kids.
Then, we used minimal distractions. We set things out the night before and used that visual so he could match things. We also devised a place where his folders could go. This all might seem trivial, but it really matters for this type of kid. The timer helps as well. You can make it a game.
Activities to Improve ADLs
- Focus on physical activity, motor skills with automaticity and incorporate aspects of yoga to increase sustained attention and memory
- Visual supports and routine with structure
- Self-talk and self-distancing strategies
- Positively reward
To improve ADLs, the key is to focus on physical activity and motor skills with the goal of automaticity. For example, we can incorporate yoga to increase sustained attention and memory. As we talked about earlier, visual supports and structured routines are other great ideas. I cannot emphasize enough the idea of self-talk. This helps with self-regulation and impulsivity on a lower level. The ability to "self-talk" should be pretty solid for kids around the age of seven, but the kids that we are talking about lack this skill. Self-distancing, or having them give strategies to someone other than themselves, is also great. Let them problem-solve and talk it through for someone else, like Batman or John Cena. This way they do not feel like they are picking on themselves or feeling pressured to figure it out for themselves. They are figuring out for someone else, and this strategy is evidence-based. We often forget to positively reward these kids. I like to do something like time with mom and dad, I develop short-term and long-term rewards with mom and dad. For example, Jeremy wanted a wrestling figure for his long term reward. But on a daily basis, he got wrestling bucks and that bought time to wrestle with dad on the weekends.
Case Study Application- Finish a Task with Necessary Supplies
Top-Down Analysis
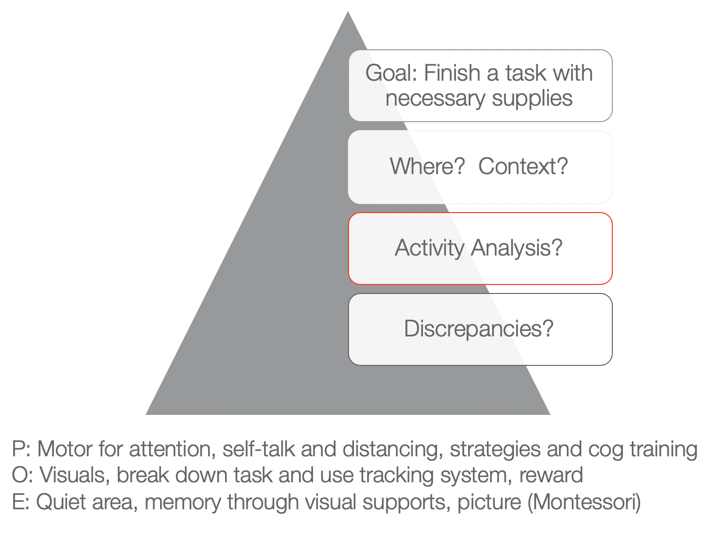
Figure 7. Example of a top-down analysis for finishing a task with necessary supplies.
The next goal is to finish a task with the necessary supplies. You can fill in whatever task that he needed to do like homework, hygiene, or whatever it was with the necessary supplies. Typically, he would start something and then not have all the supplies he needed. He would then run to go get something and then lose track of what he was doing. Activities would not get done and then there would be a mess. We want to know when this would happen and the context. What is required of that activity, and then what can he do versus what he cannot do? Those are the discrepancies.
As I stated a few moments ago, he tends to not have the needed materials. That is the first issue right out of the gate. And because he is impulsive, he starts doing something else. Eventually, he does not finish anything due to a lack of persistence and distractibility. From a personal standpoint, we could work on using motor tasks for increased attention. We know that fine motor and gross motor tasks are going to help. We could also look at using coordination tasks, self-talk, and distancing. Cognitive training is also evidence-based. Can they start to use a checklist or something to create a better strategy?
Then, from an occupation standpoint, again we can use visuals and break down the task. We can also use a tracking system that we are going to go over in just a second.
From an environmental aspect, we can encourage the use of quiet areas to help with sustained attention and better memory. Here we can also use some visual supports or a Montessori approach. "This is what the task is supposed to look like when I am finished." If we have a task, what does the end result look like so that the person knows? And even better, what are the supplies pictured so I know what I have to get first, and then I know what the end result should look like. That is super helpful for someone who is so disorganized when putting materials together.
Activities for Completing Tasks
- Inhibition: Self-talk, slowing down, self-distancing, external feedback
- WM: physical activity
- Attention: physical activity
- Using environmental strategies and visuals to support
- Behavioral: task breakdown, positive reinforcers
- Occupation-based is imperative!
We want to use occupation-based tasks, but we want them to be fun and let the child make a choice. When things are getting easier, we can then move toward less preferred tasks. For example, we do not want to start with homework.
Case Study Application: Social
- Involve a peer or sibling
- Play-based model:
- Capture intrinsic motivations (WWE)
- Empathy focus
- Arrange the environment to foster mutually enjoyable social interaction and imagination
- Teaching social play language and reading expressive body language (can use dogs and their behavior)
- Incorporate parents and coach them so they can coach outside of therapy
(Cordier et al., 2009; Wilkes-Gillan et al., 2016)
There is a play-based model that is evidence-based. They recommend involving a peer or sibling. This play-based model focuses on intrinsic motivation. With Jeremy, we could do wrestling. We could focus on empathy. It is important to arrange the environment so that it is mutually enjoyable. We need to teach social play language and reading expressive body language. The evidence was interesting as it said to use dogs because it could help the child start to read behaviors. Dogs are a little bit easier than people. Jeremy loves dogs so that would work. You could then incorporate parents in order to coach him outside of therapy. They found that to be very successful.
Case Study Application: Sleep
- Implement protocol with family and monitor
- Turn off electronics 2 hours prior
- Hot bath or shower
- PJs prepped
- Boardgame in room
- Read in bed (parents, then alone
- Highlights with organizer, feelings
- Token reward system
- Flexibility on weekends
- Sleep logs are evidence-based
- Physical activity during day imperative
(Kuhn & Floress, 2008; Fricke et al., 2006)
For sleep, this is the protocol that is highly recommended for these kids. You should turn electronics off two hours prior. Do not shoot the messenger. I know that is really easier said than done. Another protocol is to have the child take a hot bath or shower. They need to have their pajamas prepared. It is a stimulus that can help them progress through the routine. They can do a board game in the room. Another activity is reading in bed. It can start out with the parents reading and then progress to the child reading alone. They can also organize their thoughts and feelings throughout the day. It will help the brain calm down. A token reward system is another great strategy. Make sure to incorporate flexibility on the weekends. It is ok. Sleep logs are evidence-based. And again, physical activity during the day really works.
Systems and Organization
This information is what we already talked about, but I wanted to give you a good resource as well in Figure 8.
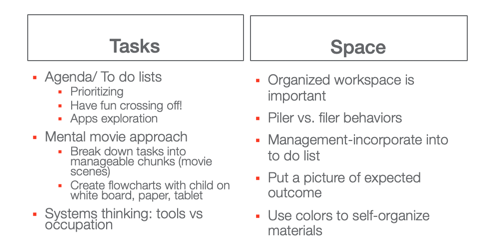
Great resource: https://www.understood.org/~/media/040bfb1894284d019bf78ac01a5f1513.pdf
Figure 8. Systems and organization examples.
I like the idea of a mental movie approach. If they are piler and not a filer, we have to appreciate that and try to use things that can help them. This may be an accordion folder or something like that.
Self-Monitoring: GOAL Attainment Scaling
This is the idea of a Goal Attainment Scale (see Figure 9). It is a strategy to identify changes in academic and social behavior. It creates habits and routines.
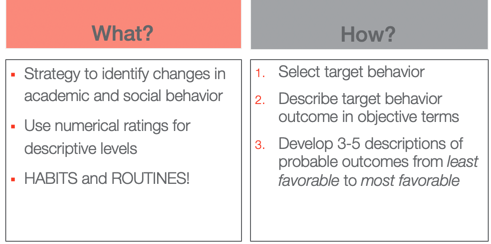
Figure 9. Goal Attainment Scale overview.
The way that you do it is you select the target behavior. You describe that behavior outcome in objective terms and then you develop three to five (I typically use five) descriptions of probable outcomes from least favorable to most favorable.
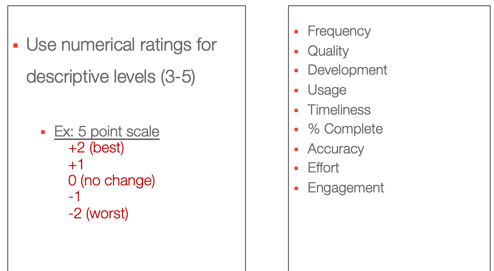
Figure 10. Numerical ratings for the Goal Attainment Scale.
These are some options that you can use, frequency, quality, usage, percent complete.
- Frequency (Never–Sometimes–Very Often–Almost Always–Always)·
- Quality (Poor–Fair–Good–Excellent)·
- Development (Not Present–Emerging–Developing–Accomplished–Exceeding)·
- Usage (Unused–Inappropriate Use–Appropriate Use–Exceptional Use)·
- Timeliness (Late–On-Time–Early)·
- Percent complete (0%–25%–50%–75%–100%)·
- Accuracy (Totally Incorrect–Partially Correct–Totally Correct)·
- Effort (Not Attempted–Minimal Effort–Acceptable Effort–Outstanding Effort)·
- Amount of Support Needed (Totally Dependent–-Extensive Assistance–Some Assistance–Limited Assistance–Independent)·
- Engagement (None–Limited–Acceptable–Exceptional)
This is what the five looks like. You have two choices. You can do a baseline here at zero or the baseline at minus two where that is the worst with no change. Or, you can start at their baseline here at two and only go up. If they cannot handle seeing that they went down, you might choose that option instead. We do not want any negative things causing them anxiety. I have also listed the actual ratings. Here is the example for our friend Jeremy in Figure 11.
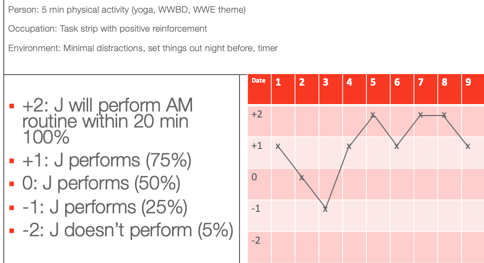
Figure 11. GAS scale example for Jeremy.
He wanted to perform his AM routine within 20 minutes according to his mom. On the first date, he was a +1, which is he did only 75% within 20 minutes. On Day 2, he had 50% of his stuff done within 20 minutes. Day three, he had only 25% done. On four, he was back up to 75%. Day five, he did everything in 20 minutes. Day six, he was back to 75%. And then you see on days seven and eight, he actually met his goal. And on day nine, he almost met his goal. Once you plot the dates you have a graph. This shows change over time and whether or not things are working. You can also do this at home to capture the change in a more specific and sensitive way. On that note, we focused on time.
Summary
Thanks for joining me today. I hope you find the information helpful. Feel free to reach out to me if you have any questions.
References
Best, J. R., & Miller, P. H. (2010). A developmental perspective on executive function. Child Development, 81(6), 1641-1660.
Cremone-Caira, A., Root, H., Harvey, E. A., McDermott, J. M., & Spencer, R. M. (2019). Effects of sleep extension on inhibitory control in children with ADHD: A pilot study. Journal of Attention Disorders, 1087054719851575.
Corkum, P., Tannock, R., & Moldofsky, H. (1998). Sleep disturbances in children with attention-deficit/hyperactivity disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 37, 637-646.
Cordier, R., Bundy, A., Hocking, C., & Einfeld, S. (2010). Empathy in the play of children with attention deficit hyperactivity disorder. OTJR: Occupation, Participation, and Health, 30(3), 122-132.
Diamond, A. (2012). Activities and programs that improve children’s executive functions. Current Directions in Psychological Science, 21(5), 335-341.
Levanon-Erez, N., Cohen, M., Traub Bar-Ilan, R., & Maeir, A. (2017). Occupational identity of adolescents with ADHD: A mixed methods study. Scandinavian journal of occupational therapy, 24(1), 32-40.
Hahn-Markowitz, J., Berger, I., Manor, I., & Maeir, A. (2016). Efficacy of cognitive-functional (Cog-Fun) occupational therapy intervention among children with ADHD: An RCT. Journal of Attention Disorders, 1087054716666955.
Faber Taylor, A., & Kuo, F. E. (2011). Could exposure to everyday green spaces help treat ADHD? Evidence from children's play settings. Applied Psychology: Health and Well‐Being, 3(3), 281-303.
Fricke L, Mitschke A, Wiater A, Lehmkuhl G. 2006. A new treatment program for children with sleep disorders – concept, practicability, and first empirical results. Prax Kinderpsychol Kinderpsychiatr 55:141–154.
Keshavarzi, Z., Bajoghli, H., Mohamadi, M. R., Salmanian, M., Kirov, R., Gerber, M., ... & Brand, S. (2014). In a randomized case–control trial with 10-years olds suffering from attention deficit/hyperactivity disorder (ADHD) sleep and psychological functioning improved during a 12-week sleep-training program. The World Journal of Biological Psychiatry, 15(8), 609-619.
Kuhn BR, Floress MT. (2008). Nonpharmacological interventions for sleep disorders in children. In Ivanenko A, ed. Sleep and psychiatric disorders in children and adolescents. New York, NY: Informa Healthcare USA Inc. pp 261–278.
Majored, M., Tüchelmann, T., & Heusser, P. (2004). Therapeutic Eurythmy—movement therapy for children with attention deficit hyperactivity disorder (ADHD): a pilot study. Complementary therapies in Nursing and Midwifery, 10(1), 46-53.
Pan, C. Y., Tsai, C. L., Chu, C. H., Sung, M. C., Huang, C. Y., & Ma, W. Y. (2019). Effects of physical exercise intervention on motor skills and executive functions in children with ADHD: A pilot study. Journal of Attention Disorders, 23(4), 384-397.
Papadopoulos, N., Stavropoulos, V., McGinley, J., Bellgrove, M., Tonge, B., Murphy, A., ... & Rinehart, N. (2019). Moderating effect of motor proficiency on the relationship between ADHD symptoms and sleep problems in children with attention deficit hyperactivity disorder–combined type. Behavioral Sleep Medicine, 17(5), 646-656.
Tandon, P. S., Sasser, T., Gonzalez, E. S., Whitlock, K. B., Christakis, D. A., & Stein, M. A. (2019). Physical activity, screen time, and sleep in children with ADHD. Journal of Physical Activity and Health, 16(6), 416-422.
Toplak, M. E., West, R. F., & Stanovich, K. E. (2017). The assessment of executive functions in attention-deficit/hyperactivity disorder: Performance-based measures versus ratings of behavior.
Tseng, M. H., Henderson, A., Chow, S. M., & Yao, G. (2004). Relationship between motor proficiency, attention, impulse, and activity in children with ADHD. Developmental Medicine and Child Neurology, 46(6), 381-388.
Wilkes-Gillan, S., Bundy, A., Cordier, R., Lincoln, M., & Chen, Y. W. (2016). A randomised controlled trial of a play-based intervention to improve the social play skills of children with attention deficit hyperactivity disorder (ADHD). PLOS one, 11(8), e0160558
Yürümez, E., & Kılıç, B. G. (2016). Relationship between sleep problems and quality of life in children with ADHD. Journal of Attention Disorders, 20(1), 34-40.
Citation
Quint, N. (2020). Pediatric case study: Child with ADHD. OccupationalTherapy.com, Article 5145. Retrieved from http://OccupationalTherapy.com
