Editor's note: This text-based course is a transcript of the webinar, The Tao Of Client-Centered OT: Deepening Your Practice, presented by Debora Davidson, PhD, OTR/L.
*Please also use the handout with this text course to supplement the material.
Learning Outcomes
- After this course, participants will be able to analyze at least three observable indicators of client-centered care.
- After this course, participants will be able to list at least three strategies to add to their client's experience of client-centeredness within their actual practice setting(s).
- After this course, participants will be able to recognize three challenges to taking a client-centered approach and ways to ameliorate or avoid them.
Introduction
I'm thrilled that so many of you are here today, eager to deepen your occupational therapy practice and explore how measurable outcomes align with client-centered care. My hope is that you leave this session feeling validated in all the work you've been doing to provide meaningful, client-centered interventions. If you're in this course, I imagine you already value client-centered care, and I hope you'll walk away feeling inspired and equipped to make it an even more intentional and routine part of your sessions.
Fawn did a wonderful job introducing my clinical background. This year marks 45 years as an OT practitioner, and my practice has continuously evolved—one of the great things about occupational therapy is that we have the opportunity to explore different paths. Throughout my career, a few central themes have remained constant: mental health care across the lifespan, working with children, teens, and adults, and occupational therapy education.
I first learned about client-centered care around 1986. At the time, I was working in a hospital, and we had a guest speaker come in to introduce this new concept. I remember feeling a little skeptical when I saw the topic. I thought, Well, of course, we care about our patients—that’s why we do this work. We’re benevolent. It wasn’t until I sat through the presentation that I had my aha moment. Client-centered care wasn’t just about caring for patients; it was something deeper—an approach that would fundamentally shape the way I practiced and, later, how I taught. That presentation, along with everything I’ve read and experienced since has influenced my work in ways I couldn’t have predicted.
Another influence on my thinking, and something we’ll touch on today, is the Tao Te Ching. My interest in it began somewhat unexpectedly in my twenties when I spotted The Tao of Pooh on my boyfriend’s bookshelf. That little red book intrigued me, and it set me on a long journey of exploring Taoist philosophy. That same boyfriend is now my husband, and over the years, I’ve explored many versions of the Tao Te Ching, from direct translations of Lao Tzu’s work to playful interpretations like The Tao of Physics and The Tao of Tea. One version I’ll reference frequently today is Getting Right with Tao by Ron Hogan—a modern, accessible translation that brings the concepts into everyday life.
Throughout this session, we’ll look at how the principles of the Tao Te Ching align with client-centered care and how they can help us refine our practice. My goal is to offer insights that are both thought-provoking and immediately useful in your work.
History
Let's start with a little history to ground us. You may remember Carl Rogers from your OT theory or foundations course. Though he wasn’t an occupational therapist, his work has influenced many professions, including ours. Rogers was an American psychologist who, over the course of his career, became frustrated with the traditional therapist role—one where the therapist was seen as the all-knowing expert, in charge of the process. He came to a different conclusion: clients are the true experts on themselves. They know what hurts, they know what they need, and they have their own definitions of a successful outcome.
Rogers coined the term client-centeredness, and we can thank him for that. He also introduced concepts like unconditional positive regard—the idea that a therapist’s respect and warmth toward a client isn’t based on their progress or any particular trait, but rather on the fundamental value of the person. He also developed active listening, which I hope was covered in your OT programs. Today, I may use that term interchangeably with therapeutic listening, but the core idea remains the same—listening in a way that ensures your understanding truly aligns with what the client is trying to communicate.
Long before Carl Rogers, there was Lao Tzu, the author of the Tao Te Ching. He was a scribe and philosopher in the Chinese court in the 6th century BCE. According to legend, he grew disillusioned with politics and the excesses of the wealthy elite, so he decided to leave the city and retreat into the wilderness. As he approached the city gates, a guard recognized him and pleaded, Master, please don’t leave without sharing your wisdom. In response, Lao Tzu wrote down his observations and reflections, which became the Tao Te Ching—a collection of insights about human nature, decision-making, and the nature of life itself.
The Tao Te Ching is full of wisdom, often laced with humor, sharp critiques, and challenges to conventional thinking. Many of its ideas have resonated with me, especially in relation to client-centered care. The word Tao literally means the path or the way, representing a universal principle that underlies everything—from the formation of galaxies to human interactions. It suggests that understanding the world isn’t just about logic; intuition plays a vital role as well.
The Tao Te Ching has been applied to many different fields—there’s the Tao of Physics, the Tao of Tea, and the Tao of Teaching. I keep thinking it would be wonderful to collaborate on the Tao of OT. After all, the Tao exists within everyone; we just have to recognize it and learn how to use it.
Client-Centered Care (CCC) As "The Way"
Everyone has client-centered care within them—we just have to tap into it. The Client-Centered Care Compass can serve as a guide in our practice. This philosophy, sometimes referred to as person-centered care, has been embedded in occupational therapy from the very beginning, even though the term itself wasn’t coined until later. The question is, why has this concept endured for so long?
If you explore the research in OT, medicine, psychology, social work, counseling, and education, you’ll see a consistent theme: a client-centered approach leads to positive change. The benefits are clear, and you’ll find articles in your resources that further support this. In many ways, client-centered care is like the Tao—difficult to define in words, but unmistakable when you see it in action.
Let’s look at some definitions from different perspectives. The OT Practice Framework: Domain and Process—a key guide for occupational therapy in the U.S.—describes client-centered care as an approach that incorporates respect for and partnership with clients, making them active participants in the therapy process. It emphasizes clients' knowledge, strengths, capacity for choice, and overall autonomy (Schell & Gillen, 2019). It’s a clear and useful definition, though I find it leaves out some of the deeper nuances of what client-centered care truly embodies.
Cole and McLean take it a step further, describing client-centered care as a collaborative approach that honors both the client’s and the practitioner’s contributions. Through interpersonal communication skills, practitioners help shift the balance of power, giving clients more control over decision-making and problem-solving. What I love about this description is that it highlights the therapist’s interpersonal skills as an integral part of the process. It also acknowledges a power shift, though it still implies that the therapist is the one “granting” that power, which suggests there’s still an inherent imbalance.
Hearing directly from clients adds another dimension to understanding client-centered care. One quote, taken from Canadian literature, captures it beautifully: "Client-centered care means that I’m a valued human being."
In Canada, client-centeredness is embedded in their national healthcare system, reinforcing its importance. Another quote always makes me smile because it reminds me of so many clients I’ve worked with:
"Why can’t I have more? Why can’t I make my own choices? How many occupations are there? There must be millions. Why am I limited to just three?"
And really—why should they be? I completely agree.
When we think about client-centered care, we recognize that it exists on different levels. Sometimes, it’s subtle, and other times, it’s more active and intentional, truly putting the client in charge. Regardless of where we work, client-centered care is a universal principle that can shape our interactions in any practice setting. If we choose to engage with it, it becomes a natural and essential part of therapeutic relationships.
Client-Centered OT Facilitates
Research and clinical experience both affirm that client-centered occupational therapy fosters many positive outcomes. It’s that moment when a client looks at you and says, "Oh, you get me." It creates a sense of connection, trust, and engagement. Clients enjoy coming to OT when they feel truly heard—when therapy reflects their values, needs, and priorities. A client-centered approach generates enthusiasm, making therapy something they look forward to rather than something they endure.
It also means that we evaluate what matters to the client and avoid wasting time on what doesn’t. Our assessments and interventions align with their concerns, and our goals are written specifically to reflect their priorities, not just standard clinical objectives. When we take a truly client-centered approach, clients gain deeper self-knowledge. They begin to articulate what they want, sometimes for the first time, because we are asking them to reflect, to consider their own goals, and to express those desires openly. Through this process, they often develop assertive communication skills—learning to advocate for themselves—because we are inviting that self-determination and reinforcing it rather than steering them toward our own agenda.
Clients in a truly client-centered setting are motivated. They’re engaged not just in the goals but in the process of achieving them. And when that happens, the outcomes are exhilarating—not just for them but also for us as therapists. It makes therapy more dynamic, more rewarding, and, ultimately, more successful.
12 Experiences of CCC
This color wheel, in Figure 1, represents twelve experiences of client-centeredness.
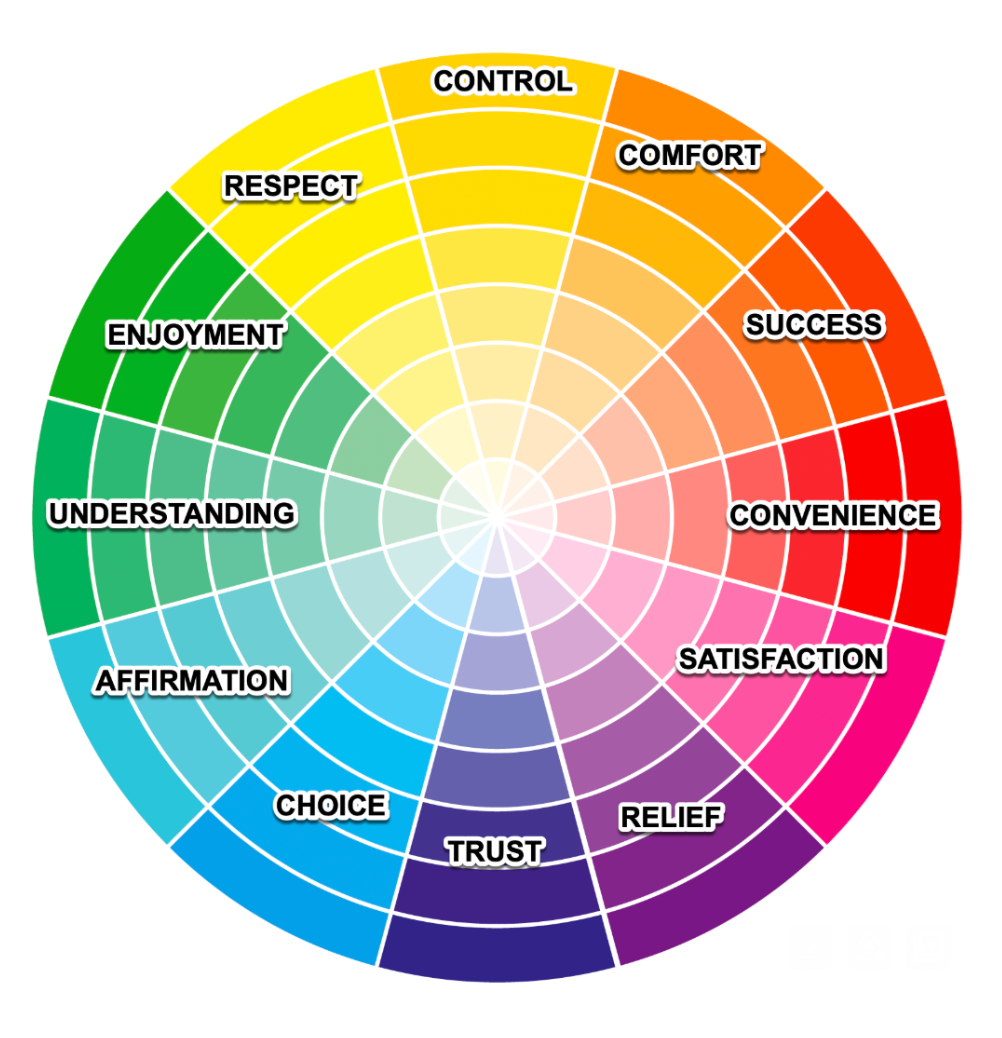
Figure 1. Graphic representation of twelve experiences of client-centered care.
When I created it, my goal was to explore what client-centeredness feels like from the client’s perspective. How do they actually experience it? That question was the foundation for this visual representation.
You’ll notice the colors shift from pale shades in the center to brighter, more saturated colors at the edges. I liked this as an analogy for the range of ways we can deliver client-centered care—sometimes in subtle, understated ways (the pale shades), and other times in more vivid, impactful ways (the brighter colors).
This is not a scientifically derived list, but rather a reflection of my own experiences with clients over the decades, combined with insights from research and literature on client-centered care. And of course, I’m sure there are more than twelve ways a person can experience client-centeredness. In fact, before I even finished this PowerPoint, I realized I had a thirteenth! I’ll slide that in later, but for now, we’re working with twelve.
I’ll be sharing examples of each, and I encourage you to engage with this in a personal way. If you’ve printed your handout, great—but if not, just grab a piece of paper. The handout itself isn’t highly detailed because my hope is that as we go along, you’ll jot down specific ideas that resonate with you—perhaps strategies for a client you’re currently working with, or insights from past experiences. My goal is for you to walk away with practical ideas that you can carry forward into your own practice.
Occupational Therapy Process/Case Study
I'm also going to discuss client-centered care through the lens of the OT Practice Framework and the OT process. In OT, we are mandated to conduct evaluations, provide interventions, and ensure that outcomes align with the person's goals at the start of therapy. I will approach the discussion from that perspective.
Additionally, to help ground and anchor the conversation, I will use a small case example. This is a fictional, very pared-down case story, but it will allow me to be more specific when discussing ways to be client-centered.
Dante
Dante is a client in my practice of Bright Futures, my private practice. I see people usually in their homes and their communities, and a lot of my clients are young to mid-age adults with neurotypical features who might also have some mental health problems. they want to be more independent, and they want to have interesting lives and not be stuck at home basically.
He's recovering from a traumatic brain injury that occurred three years ago and his parents want him to get his life on track.
Client-Centered Intake
In the initial phase of the occupational therapy process, conducting a client-centered intake is paramount. This stage serves as the foundation for building a therapeutic alliance and gathering essential information to inform subsequent interventions.
Creating a welcoming environment is crucial. I ensure that clients and their families feel at ease by greeting them warmly, offering a comfortable setting, and being punctual and prepared for our meeting. Providing my contact information and encouraging open communication fosters trust and signals my commitment to their well-being.
During this initial interaction, I clearly outline what clients can expect from the therapy process. This includes discussing the collaborative nature of our work, potential assessments, and the roles we will each play. Emphasizing that I view them as active participants—essentially as my "employers"—reinforces a sense of agency and partnership.
Collecting demographic details such as name, address, and date of birth is standard practice. Beyond these basics, understanding the specific concerns and expectations of both the client and their family is vital. I inquire about their reasons for seeking occupational therapy and their understanding of the process. This dialogue helps in assessing the suitability of my services and identifying initial areas for evaluation.
Approaching each client with humility allows me to remain open and receptive to their unique experiences and perspectives. This mindset encourages me to prioritize their comfort, adjust the pacing of our sessions to meet their needs, and acknowledge any missteps on my part. Being willing to apologize and correct course as necessary demonstrates respect and fosters a stronger therapeutic relationship.
Cultural sensitivity is integral to this process. I am attentive to preferred titles and pronouns, and I respect cultural norms regarding eye contact and communication styles. For instance, if a client is uncomfortable with direct eye contact, I adjust my approach to ensure they feel at ease.
Adhering to the principle of "nothing about me without me," I involve clients in all decisions regarding their care. Before reaching out to other professionals or family members, I seek the client's permission and discuss the purpose of such communications. This practice not only respects their autonomy but also reinforces their central role in the therapeutic process.
In summary, the client-centered intake phase is a critical component of occupational therapy, setting the stage for a collaborative and effective therapeutic journey. By focusing on rapport-building, clear communication, humility, cultural sensitivity, and client autonomy, I strive to create a strong foundation for meaningful and personalized care.
Setting the Vibe for CCC
Establishing a client-centered therapeutic environment begins with authentic warmth and active listening. When meeting clients, I express genuine pleasure in our encounter, adjusting my demeanor to match their emotional state—remaining warm yet mirroring their energy level to foster comfort.
I initiate our dialogue by asking, "What would you like to work on?" This open-ended question invites clients to share their priorities. Practicing active listening, I pose concise questions, allow ample time for responses, and then paraphrase their input to ensure accurate understanding. For instance, I might say, "From what you've shared, it seems you're feeling overwhelmed by daily tasks. Is that correct?" This approach not only clarifies their concerns but also validates their experiences.
It's not uncommon for clients to express profound appreciation during these sessions, sometimes even becoming emotional, as they feel truly heard—perhaps for the first time by a professional. Such moments underscore the impact of genuine listening in building trust.
I reassure clients by affirming, "You've come to the right place," especially when they express feelings of emptiness or embarrassment about their current situation. Emphasizing that my role is to assist them in identifying and engaging in meaningful activities helps alleviate their concerns.
A central tenet of my practice is conveying, "I work for you." This statement empowers clients, positioning them as active participants in their therapeutic journey. While some may initially find this dynamic unfamiliar, they often grow to appreciate and embrace the collaborative nature of our relationship.
Building trust and respect is a reciprocal process. By demonstrating genuine interest, providing empathetic responses, and maintaining transparency, I create a foundation where clients feel valued and understood.
As Thich Nhat Hanh wisely noted, "For things to reveal themselves to us, we need to be ready to abandon our views about them." This perspective encourages openness and receptivity, essential qualities in truly understanding and supporting our clients.
Client-Centered Evaluation
In the client-centered occupational therapy evaluation process, the paramount question to address is: "What do you want most from our work together?" This inquiry delves into the client's primary goals and aspirations, forming the foundation for a personalized and meaningful intervention plan.
Uncovering a client's true desires, or "heart's desire," is essential, though it may require time and trust-building. For instance, a client like Dante might initially express a desire to move out of his parents' house, seek employment, or establish social relationships. Understanding these core motivations enables the therapist to tailor interventions that resonate with the client's personal goals.
Equally important is identifying barriers that hinder the client's progress. Engaging both the client and their support system in discussions about perceived obstacles provides a comprehensive perspective. In Dante's case, his parents might observe a shift in behavior post-accident, noting increased inactivity and altered routines, while Dante himself might feel pressured by their expectations. Recognizing these dynamics is crucial for developing effective strategies that address both environmental and personal factors.
Throughout the evaluation, embodying values such as trust, authenticity, and transparency fosters a collaborative atmosphere. Clearly explaining the purpose and process of each assessment tool, and seeking consent before involving others, ensures that the client feels respected and in control. Providing choices within the evaluation process empowers clients, enhancing their engagement and commitment to therapy.
Affirming the client's strengths and validating their desires reinforces a positive self-concept and motivates progress. Emphasizing a strengths-based approach, as outlined in the Occupational Therapy Practice Framework, allows clients to leverage their capabilities in overcoming challenges. Ensuring confidentiality and discussing its boundaries further solidifies the therapeutic alliance, creating a safe space for open communication.
In summary, a client-centered evaluation prioritizes understanding the client's deepest aspirations and the obstacles they face. By integrating core values and ethical principles, therapists can develop tailored intervention plans that align with the client's personal goals, fostering meaningful and sustainable outcomes.
Some Tools & Methods to Facilitate CC Evaluation
Incorporating client-centered evaluation tools is fundamental to developing effective and personalized intervention plans in occupational therapy. These tools facilitate a comprehensive understanding of a client's daily routines, self-perceptions, and personal goals, ensuring that therapy aligns with their unique needs and preferences.
Daily Activities Interview. Initiating the evaluation process with a Daily Activities Interview provides valuable insights into a client's typical day. By asking open-ended questions about their daily routines—such as their usual wake-up times and subsequent activities—we can assess the level of structure or variability in their schedule. This understanding helps identify areas that may benefit from intervention, such as establishing consistent routines or introducing new, meaningful activities.
Canadian Occupational Performance Measure (COPM). The COPM is a widely recognized, client-centered assessment tool that involves a semi-structured interview. Clients identify daily activities they need or want to do and rate the importance, performance, and satisfaction associated with these activities. This process highlights areas of difficulty and prioritizes them based on the client's perspective, ensuring that the therapy focuses on what matters most to the individual.
Occupational Self-Assessment (OSA). The OSA, grounded in the Model of Human Occupation, is a self-report tool that captures clients' perceptions of their occupational competence and the value they place on various activities. Clients rate their performance in areas such as personal care, meal preparation, and social interactions and the importance of these activities in their lives. This assessment facilitates collaborative goal-setting and prioritization, empowering clients to take an active role in their therapeutic journey.
Service Menu. Developed specifically for the Bright Futures program, the Service Menu is a personalized tool that allows clients to express their preferences for areas they wish to address in therapy. Clients indicate their interest and prioritize topics such as job skills development, educational planning, internet usage for information gathering, establishing exercise routines, and finding social connections. This approach positions clients as active participants in their therapy, reinforcing the notion that they are effectively employing their therapist to assist in achieving their personal goals.
Interest Checklist. Utilizing an Interest Checklist can further enhance the client-centered evaluation by identifying activities that the client enjoys or is interested in pursuing. This information is invaluable for tailoring interventions that are both engaging and meaningful, thereby increasing the likelihood of successful outcomes.
Participatory Activity Observations. Engaging clients in participatory activities—such as cooking a meal together, visiting a café, or exploring a library—provides real-time observations of their skills, preferences, and potential challenges. These shared experiences offer practical insights that inform the development of relevant and effective intervention strategies.
Incorporating these tools and methods fosters a collaborative and empowering therapeutic environment. By actively involving clients in the evaluation process, we not only gain a comprehensive understanding of their needs and desires but also promote a sense of ownership and motivation toward achieving their therapeutic goals.
Client-Centered Goal Setting
Incorporating client-centered goal setting into therapy is essential for fostering a sense of control and ownership in clients over their intervention plans. This collaborative approach not only enhances motivation but also leads to more meaningful and personalized therapeutic outcomes.
Presenting a draft intervention plan to clients as a starting point for discussion is a practical strategy. By explicitly stating that the plan is a draft and actively seeking their feedback, clients are encouraged to voice their preferences and concerns. This process ensures that the intervention aligns with their personal goals and values, adhering to the principle of "nothing about me without me." Such transparency and collaboration are fundamental to client-centered care.
When discussing evaluation results and translating them into therapeutic goals, it's crucial to highlight and incorporate the client's strengths. Supporting the client's opinions while blending in professional expertise fosters a balanced and respectful therapeutic relationship. For example, if a client like Dante expresses interest in a challenging career, such as air traffic control, the approach would involve exploring this aspiration together. Researching the requirements and daily realities of the profession can help the client make an informed decision. This method respects the client's autonomy and supports self-efficacy.
Ensuring that the client's true hopes and desires are embedded within the intervention plan is vital. Communicating that the plan is adaptable and subject to change as therapy progresses reinforces the client's sense of control. Regular check-ins to assess the plan's relevance and effectiveness allow for timely adjustments, ensuring the therapy remains aligned with the client's evolving goals.
An intervention plan that genuinely reflects the client's authentic self is inherently motivating. Clients are more likely to engage actively in therapy when they see their personal goals and values mirrored in the treatment plan. This alignment fosters excitement and a proactive attitude toward therapeutic activities.
Assisting clients in developing assertive and respectful communication skills is another facet of client-centered care. Preparing clients for interactions with parents, teachers, or employers by rehearsing meetings or presentations can boost their confidence and autonomy. For instance, helping a high school client create a PowerPoint presentation for an Individualized Education Program (IEP) meeting can transform their passive participation into active engagement, allowing them to convey their progress and goals effectively.
Therapists must recognize the importance of focusing on aspects within their control and avoid exerting undue pressure on the therapeutic process. As highlighted in the Taoist philosophy, "The master doesn't worry about what they can't control; that's why they're always satisfied." This perspective encourages therapists to facilitate a supportive environment where clients feel empowered to pursue their goals, understanding that the client's active participation is key to successful outcomes.
In summary, client-centered goal setting involves a collaborative, flexible, and empowering approach that respects the client's autonomy and integrates their strengths and aspirations into the therapeutic process. This methodology not only enhances client satisfaction and motivation but also leads to more effective and meaningful therapeutic outcomes.
Client-Centered Intervention
Intervention is a pivotal phase in Dante's therapeutic journey. He has expressed a desire for meaningful friendships and improved leisure activities, noting that he often sleeps excessively during the day and engages in repetitive, unstimulating tasks. Through our discussions, Dante has identified a goal to establish a regular exercise routine and has become receptive to adjusting his day-night schedule. This adjustment aims to prepare him for independent living and a future career. These objectives will guide our treatment plan.
From a safety perspective, I've observed that Dante occasionally exhibits impulsive behaviors, leading to unwise decisions. His social skills are inconsistent; at times, he makes remarks that others find startling or offensive. Additionally, Dante frequently needs immediate access to restroom facilities, often leaving sessions abruptly to accommodate this urgency. This pattern suggests a possible underlying medical issue. Therefore, I plan to guide his family toward consulting a healthcare professional to evaluate the cause of his frequent and urgent need to urinate.
Addressing these concerns through a client-centered approach is essential. One of the profound contributions occupational therapy offers is relief. For clients experiencing physical discomfort, we employ modalities and positioning strategies to alleviate pain. In Dante's case, alleviating boredom is crucial. By introducing engaging activities, we can instill hope and optimism, counteracting negative self-talk and reducing feelings of isolation and loneliness. Our sessions serve as a vital social interaction, especially for someone who has been homebound and solitary. However, it's important that these sessions are a means to an end, promoting broader social engagement beyond our meetings.
Celebrating successes, no matter how small, is a cornerstone of this process. I make it a point to highlight Dante's achievements, noting improvements such as waking up earlier or maintaining daily hygiene routines. Recognizing these milestones fosters a sense of competence and motivates further progress.
Enjoyment is another critical element. I strive to make our sessions enjoyable, incorporating laughter and introducing pleasant surprises or novel activities to prevent monotony. By aligning our activities with Dante's interests, we create a more engaging and effective therapeutic experience.
Safety remains a constant priority. I continuously assess Dante's tolerance levels, determining when to introduce new challenges or when to allow for rest. As the Taoist philosophy suggests, sometimes it's beneficial to pause and observe, allowing for organic progress. Incorporating moments of relaxation within our sessions provides Dante the space to reflect and grow at his own pace.
In summary, by focusing on relief, celebrating successes, ensuring enjoyment, and maintaining safety, we can create a holistic and client-centered intervention plan that addresses Dante's unique needs and fosters his personal development.
Client-Centered Discharge (Outcomes)
The final phase of therapy, discharge, holds significant importance in the therapeutic journey. I prefer to approach this phase with a sense of formality, dedicating an entire session to focus solely on the discharge process. This allows for a meaningful conclusion to the therapeutic relationship.
For instance, with a client like Dante, I would organize a special final session. Depending on his preferences, I might bring a cupcake or, if he favors savory treats, perhaps a burrito. This gesture adds a personal touch to our concluding meeting.
During this session, I actively seek feedback by asking questions such as, "How do you think this work went?" and "What did you achieve?" I encourage clients to share what they appreciated about our work together and to discuss any difficulties or aspects they wish had been different. This open dialogue fosters a comprehensive review of their progress, highlighting the journey from where we began to where they are now.
Celebrating these successes is crucial. I affirm and reassure clients about their readiness to transition away from regular sessions, expressing gratitude for the opportunity to be part of their journey. It's a privilege to witness and contribute to their growth, and I make it a point to thank them for teaching me and allowing me to assist in their progress.
Reflecting on this process, I'm reminded of the saying, "The master doesn't give orders but works alongside others. When the job is done, people are amazed at what they've accomplished." This resonates deeply with me, as the goal is for clients to feel ownership of their achievements. It's gratifying to hear clients remark that they felt capable all along, as it underscores their empowerment and the effectiveness of a collaborative therapeutic approach.
I recognize that as you listen, you're contemplating your own practice and the nuances of therapy in your specific context. Embracing a thoughtful and personalized discharge process can enhance the therapeutic experience, leaving a lasting positive impact on both the client and the therapist.
Challenges to CCC
I understand that implementing client-centered care is challenging. Many therapists, supported by literature, find it difficult or even impossible to practice client-centered care in their specific settings due to various obstacles.
Time pressures and productivity demands often hinder our ability to focus entirely on the client's needs. Rigid and rejectionist protocols can further constrain our flexibility, making it tough to adapt to individual client preferences. Anxiety plays a role, too—both ours and the client's. I sometimes worry about uncovering issues I might not be equipped to address, while clients may fear expressing their desires, be concerned about being rebuffed, or face the impossibility of achieving what they truly want.
Cultural pressures add another layer of difficulty. I've experienced situations where colleagues laughed at the notion of allowing clients to make their own choices, with remarks like, "Don't you get it? They're mentally ill; they can't decide." Such attitudes are offensive to me and highlight the need for courage in advocating for our clients. I make it a point to involve the client directly, stating, "I'm going to ask the client," or "This is not what he wants," and ensuring we pause discussions to give the client a chance to voice their perspective.
I firmly believe in the effectiveness of client-centered care. In my experience, it surpasses therapy-driven, therapist-driven, or even family-driven approaches. Embracing this method requires a thick skin and confidence in its validity—it's not a cop-out. Advocacy is often necessary, whether it's requesting budget allocations for custom items tailored to a client's needs or securing appropriate physical spaces conducive to their goals.
For instance, teaching clients to cook without access to a traditional kitchen has been a recurring challenge. Through creative solutions, like utilizing a plug-in electric skillet or a microwave, we've managed to overcome such obstacles.
I acknowledge the difficulties posed by time constraints, which is why I've developed the habit of therapeutic listening. This practice allows me to efficiently understand and address client concerns without unnecessary prolongation. Building a network of co-professionals for referrals is also crucial, ensuring that clients receive comprehensive support beyond my expertise as an occupational therapist.
Rewards/Outcomes of CCC
Embracing client-centered care is undoubtedly challenging, but the rewards are profound. I've witnessed firsthand the transformative outcomes it brings. Clients not only receive meaningful interventions and evaluations but also depart with a renewed sense of self-determination and enhanced skills to sustain it. Their families, teachers, and peers begin to see them in a new light. As clients gain confidence and autonomy, their happiness grows—and so does mine. This approach fosters a shared sense of fulfillment among all involved.
Intentionality is key to evolving as client-centered practitioners. Each day and in every session, I consciously commit to this approach, striving to remain open-minded, humble, and empathetic. Expressing these qualities authentically, coupled with consistent therapeutic listening, forms the foundation of my practice.
Developing a diverse toolkit of techniques and creative strategies is essential for tailoring assessments and interventions to each client's unique context. This customization ensures that our methods resonate with their individual experiences and environments. Embracing this path requires courage—the willingness to stand firm in client-centered principles, even if it invites skepticism or misunderstanding from others.
While client-centered care may be difficult to encapsulate fully in words, its presence is unmistakable in practice. When we engage in it, we recognize its impact intuitively, witnessing the genuine connections and positive changes it fosters.
Summary
Everyone has tao in them, they just have to use it. I hope our conversation has left you with a refreshed appreciation for the power of client centered care and a sense of commitment for providing it. And maybe a few ideas for ways that you know you might try in your practice.
Exam Review
1)What is a key principle of client-centered care, as described in the presentation?
2)Which of the following is an example of a tool or method to facilitate client-centered evaluation?
3)What outcome is associated with client-centered discharge planning?
4)What is one challenge to implementing client-centered care mentioned in the presentation?
5)According to the presentation, what interpersonal approach is essential for client-centered care?
References
See additional handout.
Citation
Davidson, D. (2025). The tao of client-centered OT: Deepening your practice. OccupationalTherapy.com, Article 5783. Retrieved from https://OccupationalTherapy.com
